Medical Bill Auditing Services: Recover Revenue
Medical bill auditing services are a specialized process for systematically reviewing claims to find and recover lost revenue from billing errors, underpayments, and compliance gaps. That matters because 80% of medical bills contain at least one error according to a 2026 industry report cited by ClinicMind's medical billing statistics roundup.
For a physician owner, that statistic isn't abstract. It shows up as avoidable denials, preventable write-offs, slow payer follow-up, and A/R that stays older than it should. A real audit looks for where money leaks out of your revenue cycle. It checks whether your documentation supports the CPT code billed, whether modifiers were used correctly, whether charge capture failed upstream, and whether payer edits are systematically suppressing reimbursement.
Practices usually call for an audit when collections feel soft or denials spike. In my experience, that's often late. The better use of auditing is earlier and more strategic. Done well, it becomes a revenue recovery and optimization tool that helps you collect what you already earned.
What Are Medical Bill Auditing Services
Medical bill auditing services are a structured review of how your practice captures charges, documents services, codes encounters, submits claims, and follows payer rules. The point isn't to create another compliance binder. The point is to find where earned revenue is being lost and put controls in place so the same mistakes don't keep repeating.
For an owner, the practical question is simple. Are you getting paid correctly and quickly for the care you already delivered? If the answer is uncertain, your billing operation needs more than staff effort. It needs independent review.
A useful audit traces the claim from chart to payment. That includes documentation support, CPT and ICD-10 selection, modifier use, charge posting, payer edits, and the appeal path when a claim is denied or downcoded. If you want a broader operational frame for where auditing sits in the business, this overview of revenue cycle management is a good reference.
What practice owners often miss
Owners rarely lose sleep over a single wrong modifier. They lose sleep over the cumulative effect of dozens of small misses every week.
- Missed charges: A service was performed, documented partially, but never posted as a charge.
- Undercoding: The documentation supported a higher level or separate payable service, but the claim went out conservatively and stayed that way.
- Incorrect modifiers: Modifier 25, 59, 76, or anesthesia modifiers can make the difference between payment and denial.
- Payer mismatch: The claim may be coded correctly under CMS logic but still fail a commercial payer edit.
Practical rule: If your team can't explain why a denial keeps recurring, you don't have a one-off problem. You have a process problem.
A modern audit also has to account for automation. Practices that want to understand how AI is shaping high-volume review work can look at examples of finance industry AI agents, because the same operational idea applies here. Technology can help surface exceptions faster, but it doesn't replace specialty judgment or payer-specific nuance.
What a good audit changes
A strong audit should improve three business outcomes:
- Cash flow improves because fewer claims sit unresolved.
- Denial pressure drops because recurring defects get fixed at the source.
- Owner visibility improves because you can see which specialties, providers, or payers are driving leakage.
That's why practices that treat auditing as a revenue function usually get more value from it than practices that treat it as a compliance task.
The Two Core Audit Methodologies
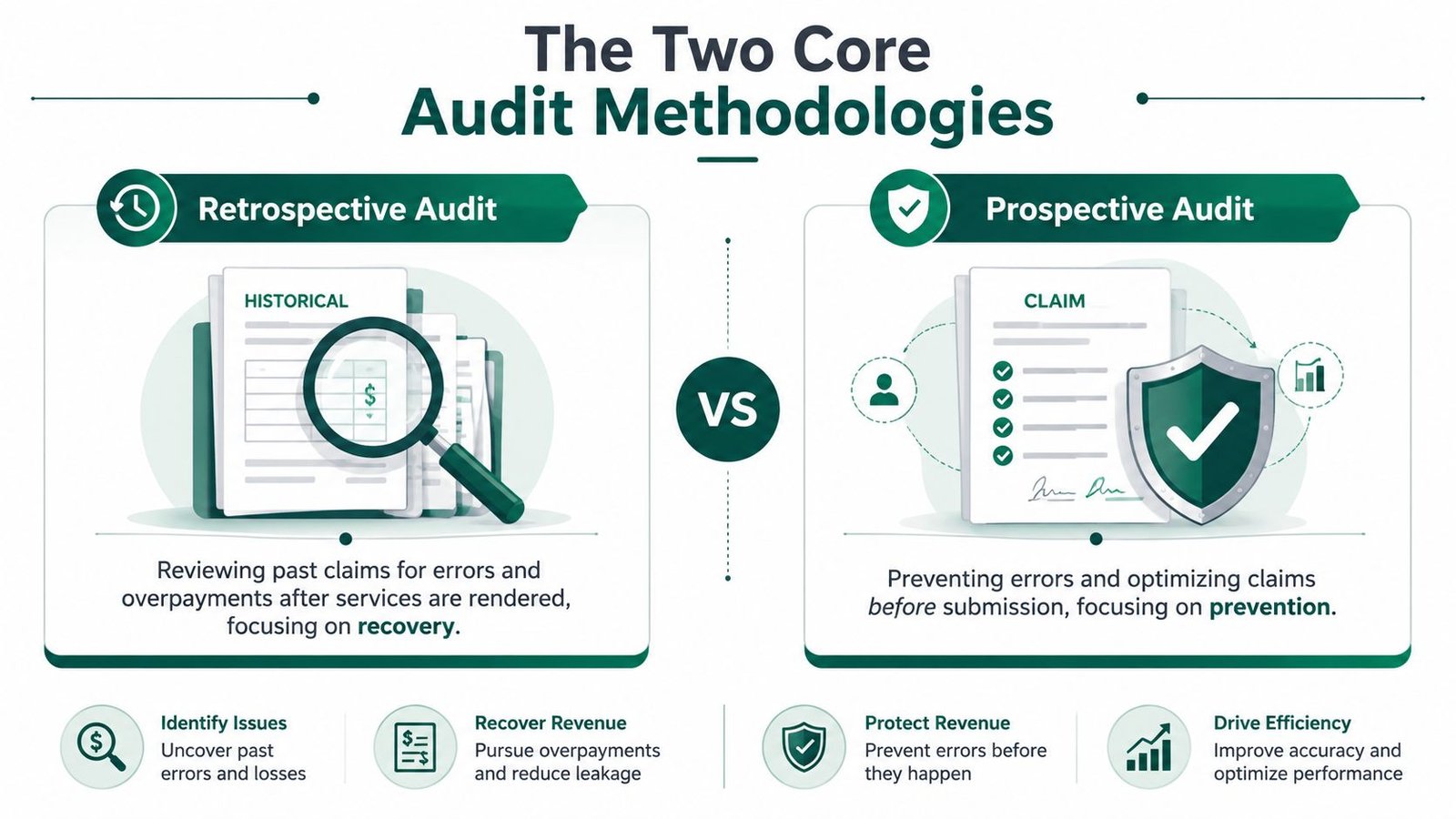
The two core models are retrospective and prospective audits. Most independent practices eventually need both, but they solve different problems.
A retrospective audit looks backward. It reviews claims already billed, paid, denied, or written off to identify patterns such as underpayments, missed modifiers, weak documentation, or payer behavior that your team didn't challenge. This is the right model when you suspect money has already leaked out of the system.
A prospective audit looks forward. It reviews claims before submission or before final release to catch preventable errors while they're still fixable. This is the right model when your priority is reducing rework and preventing denials from entering A/R in the first place.
Retrospective versus prospective in practical terms
Think of retrospective review as reading the autopsy report. Think of prospective review as checking the aircraft before takeoff. One explains where revenue already went wrong. The other protects future revenue from avoidable damage.
| Attribute | Retrospective Audit | Prospective Audit |
|---|---|---|
| Primary goal | Recover missed or lost revenue and find patterns | Prevent denials and clean up claims before submission |
| Timing | After claim submission, payment, or denial | Before claim submission or final billing release |
| Best use case | Underpayments, appeals, payer takebacks, chronic write-offs | Front-end edits, modifier issues, missing documentation |
| Main output | Findings report, root-cause analysis, recovery opportunities | Pre-bill corrections, cleaner claims, fewer preventable denials |
| Owner benefit | Identifies what was lost | Protects what should be collected next |
If your group is already struggling with recurring rejections, this guide to medical billing denial management pairs naturally with the audit decision.
When each methodology works best
A retrospective audit works best when:
- You've changed billers or vendors recently: Transition periods often hide underpayments and unresolved denial backlogs.
- A payer suddenly looks less profitable: The issue may be fee schedule variance, claims edits, or appeal failures.
- Provider productivity feels disconnected from collections: That usually signals leakage between charge entry and reimbursement.
A prospective audit works best when:
- New providers join the practice: Their documentation habits often differ from established workflows.
- You've added new services or procedures: New CPT families and payer rules create immediate risk.
- Your team is appealing too much routine work: That's a sign claim defects are entering the system too early.
Prospective audits save administrative effort. Retrospective audits recover what slipped through. Practices with high claim volume usually need a loop between the two.
Anatomy of a Professional Bill Audit
A professional audit is much more rigorous than sampling a few EOBs and calling it done. As described by PHC's overview of medical billing audit work, a technically sound audit is a line-by-line validation of claim fields against the medical record, payer rules, and coding standards to detect upcoding, unbundling, modifier misuse, and charge errors before payment is finalized.
That matters because claim failure is usually specific. It's not “billing is messy.” It's that CPT 93458 was billed without documentation that supports the full service set, or modifier 59 was used where NCCI logic points to a more appropriate modifier, or a postoperative visit was billed separately during a global period with no support for modifier 24.
Step one through three
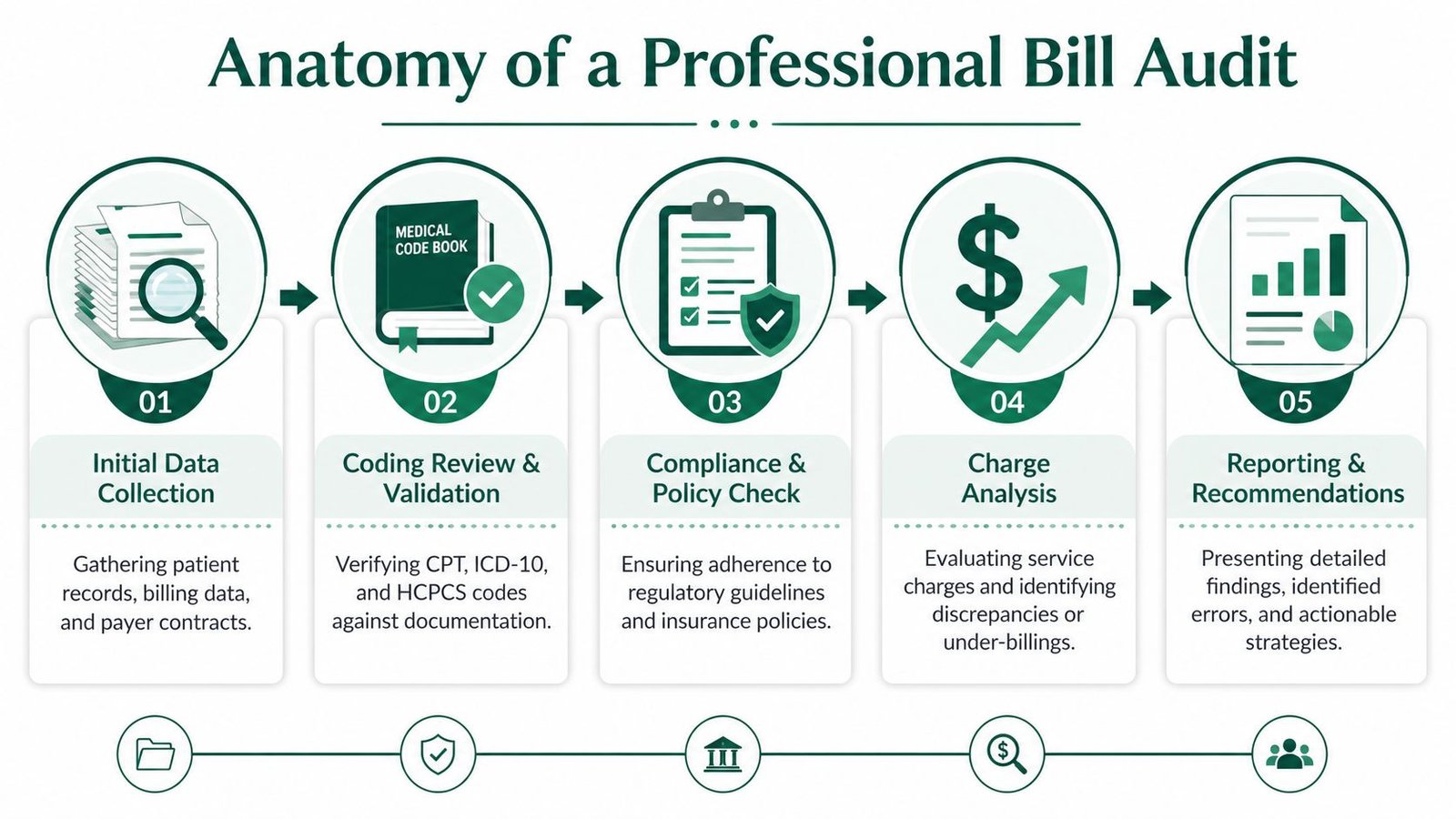
The first stage is data scoping. The auditor pulls a targeted mix of encounters by provider, payer, location, denial category, and high-risk service line. Broad random sampling has some value, but the best recovery work usually happens where the dollars and complexity are concentrated.
The second stage is chart-to-claim validation. The auditor checks whether the documentation supports the CPT, HCPCS, and ICD-10 codes billed. For physician owners, this stage reveals both underbilling and overbilling. A note may support a separate procedure that was never charged, or it may fail to support a modifier that triggered a denial.
The third stage is payer rule matching. CMS guidance, NCCI edits, local coverage expectations, and payer-specific medical necessity rules all matter. A claim can be clinically accurate and still fail because it doesn't match a payer's edit logic.
Step four and five
The fourth stage is charge integrity review. In this stage, strong audits outperform basic coding checks. They look for missing charges, duplicate charges, incorrect unit counts, and services that were documented but never made it to the claim.
The fifth stage is financial mapping and corrective action. A useful report doesn't just list defects. It ties each defect to an operational fix, such as provider education, template changes in the EHR, front-desk eligibility controls, or biller retraining on modifier selection.
A solid deliverable set usually includes:
- Executive summary: The owner-level view of what's hurting collections and where the biggest recovery opportunities sit.
- Claim-level findings: Specific errors tied to claim examples, payers, providers, and service lines.
- Root-cause analysis: Why the error happened, not just what happened.
- Action plan: The workflow, training, and system changes required to stop recurrence.
The best audit reports read like a management tool, not a coding lecture.
What good auditors look for in real claims
Auditors tend to focus on predictable failure points:
- Modifier misuse: Modifier 25 for a same-day E/M service, modifier 59 for distinct procedural service, modifier 76 for repeat procedure, and anesthesia modifiers tied to medical direction or medical supervision.
- Bundling errors: Unbundled component billing where an all-inclusive CPT already includes the work.
- Global-period mistakes: Billing follow-up care separately when it's included, or missing a legitimate modifier 24 or 79 when separate payment is appropriate.
- Unit and time issues: Especially in anesthesia, infusion, and therapy-related workflows.
That's where revenue is won or lost. Not in abstract audit theory, but in claim mechanics.
Common Billing Pitfalls by Medical Specialty
Specialty blind spots are where generic billing advice fails. The same billing team can look competent in a low-complexity office and still leak money badly in anesthesiology, cardiology, orthopedics, pain, or behavioral health. A useful audit knows where your specialty creates friction between documentation, coding, and payer edits.
One of the most overlooked issues is what Fox Group notes about billing audits: audits can uncover services provided but not recorded as charges, along with denials tied to frequency and diagnosis limits. That's an owner problem, not just a coder problem, because it directly affects collected revenue.
Anesthesiology
Anesthesia billing lives and dies on unit accuracy, start-stop time integrity, concurrency, and modifier discipline. If your team misstates time units, applies the wrong physical status modifier, or mishandles medical direction requirements, the claim may pay incorrectly or invite post-payment scrutiny.
A common issue is modifier confusion around medically directed versus supervised cases. Another is documentation that supports anesthesia care generally but doesn't support the exact billing structure used. We've also seen practices misuse modifier 23 for unusual anesthesia when the record doesn't clearly justify it.
For an owner, the takeaway is simple. In anesthesiology, “close enough” billing is expensive because errors repeat across many cases. Practices in this space need specialty-specific workflows, not generalist review. The same is true in other high-complexity service lines such as orthopedic billing services, where procedural rules can be equally unforgiving.
Cardiology
Cardiology groups often leak revenue in the gap between diagnostic services and interventional coding. A claim for a diagnostic catheterization, imaging interpretation, or stress-related service may be technically submitted, but the documentation may not support separate components the way the practice expected.
Examples owners should recognize include:
- CPT 93000, 93005, and 93010: The global ECG service versus tracing-only and interpretation-only distinctions matter. If workflow ownership is unclear, one component may never be billed.
- CPT 93458 family: Cardiac cath coding requires tight alignment between operative documentation and the exact services reported.
- Modifier use on multiple same-day procedures: Incorrect modifier logic can collapse payment when the work was distinct and payable.
A cardiology audit should test whether your billers understand not just the codes, but the payer behavior around them.
In cardiology, a coding review without a documentation review misses half the problem.
Orthopedics and pain
Orthopedics creates trouble around global periods, fracture care packages, implants, and distinct procedural services. Modifier 59 often gets used too aggressively or too lazily. Both are costly. If your team appends it routinely without chart support, you create compliance exposure. If they avoid it even when distinct services were performed, you leave money uncollected.
Pain management has similar pressure points. Injection coding, imaging guidance, laterality, and repeat service logic all require precision. Owners usually see the downstream symptom first, such as repeated payer denials or high manual appeal volume.
Behavioral health and other outpatient specialties
Behavioral health revenue often stalls because authorization management and frequency limits aren't integrated tightly with billing operations. A clean claim can still fail if the underlying visit wasn't aligned to the payer's authorization and diagnosis requirements.
Dermatology, pediatrics, and internal medicine have their own versions of the same issue. Lesion procedures, vaccine administration, preventive versus problem-oriented E/M distinctions, and age-specific service documentation all create opportunities for both denials and missed charges.
The common thread across specialties is this: the highest-value audit doesn't only ask whether the code was technically correct. It asks whether your practice captured every payable service, documented it properly, and defended it under the payer's rules.
Measuring the ROI of Auditing Services
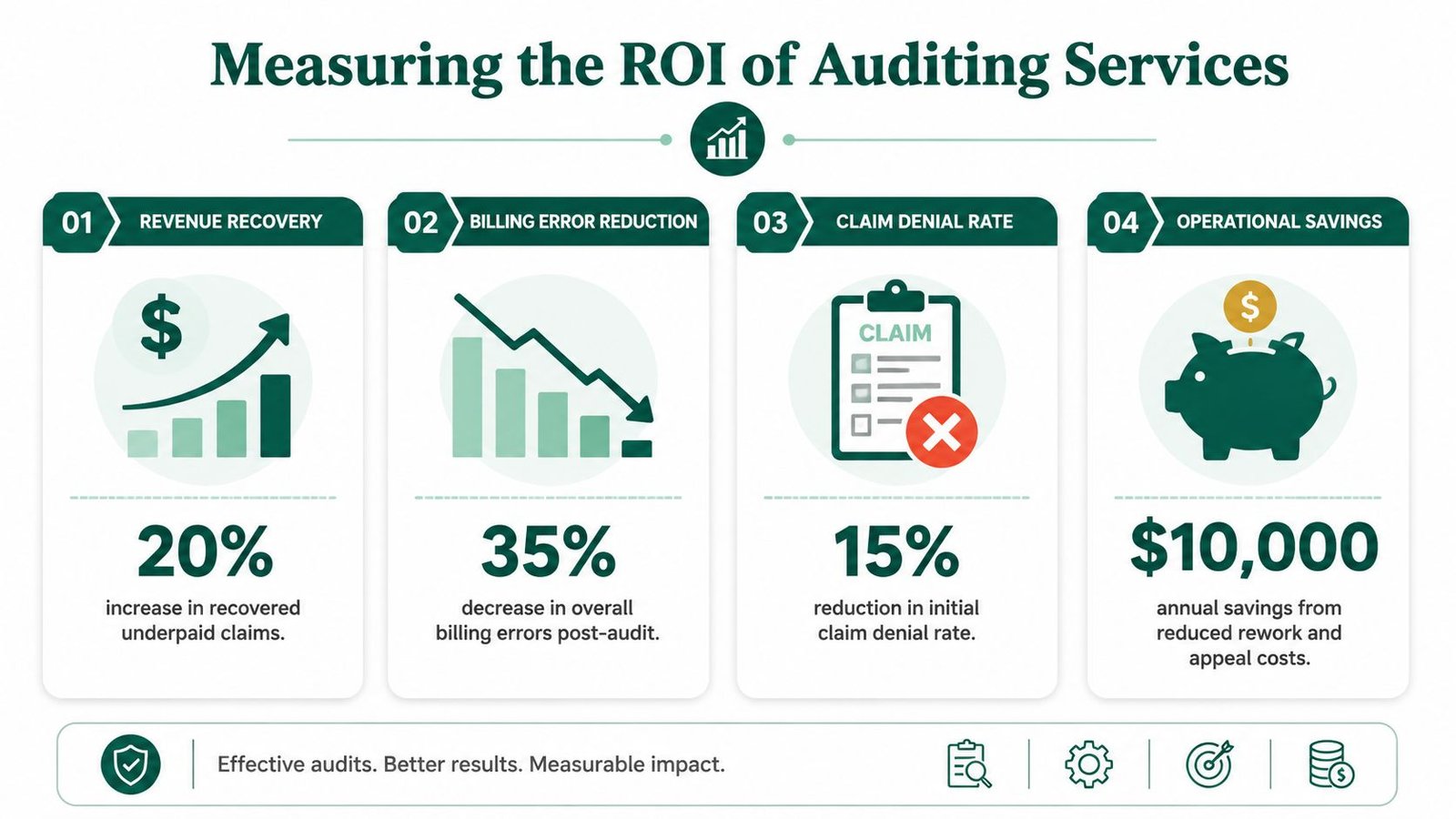
An audit has value only if it changes financial performance. The actual return isn't the report. It's what happens after the findings are converted into workflow changes, cleaner claims, stronger appeals, and fewer repeated mistakes.
That's why the most effective audit programs “close the loop.” As explained by CBS Medical Billing's discussion of audit workflows, auditors review claims, EHR documentation, payer-specific requirements, and root causes of rejection, then feed those findings back into staff training and process redesign. That's the difference between a static review and a working revenue control.
If you're comparing in-house fixes to vendor support, this breakdown of medical billing outsourcing costs helps frame the financial decision.
What owners should track
Practice owners don't need a complicated scorecard. They need a short list of metrics tied directly to cash.
- Denial pattern by category: Not just total denials, but recurring root causes such as authorization, modifier, eligibility, or medical necessity.
- A/R aging movement: Are preventable delays shrinking after corrections are implemented?
- Net collections consistency: Are you collecting more of what was contractually and operationally collectible?
- Recovered or prevented leakage: This includes corrected underpayments, saved write-offs, and cleaner future claims.
A practical ROI framework
Use a before-and-after lens.
First, identify which defects are consuming the most money or staff time. That may be repeated modifier denials, undercoded office procedures, missing charges, or weak appeal documentation. Next, assign responsibility for the fix. Some issues belong with providers, some with front office staff, some with coders, and some with the billing vendor.
Then look for three signs that the audit is paying off:
- The same denial categories stop recurring.
- Claims move through A/R with less manual rescue work.
- Your team spends more time resolving true exceptions and less time reworking routine defects.
Owner lens: If your audit doesn't lead to staff retraining, template changes, or payer-specific edits, you bought information, not improvement.
The strongest ROI often comes from preventing future leakage, not just recovering old dollars. That's why a good audit program becomes part of operations rather than an isolated project.
How to Choose the Right Auditing Partner
Choosing an auditing partner is less about who promises the most and more about who can operate at your specialty's level of complexity. In a simple primary care environment, many vendors can produce a decent compliance review. In anesthesiology, cardiology, orthopedics, or behavioral health, the wrong partner will miss the very issues costing you money.
That challenge is getting harder because payer scrutiny is becoming more automated. As noted by MedReview's discussion of hospital bill audits and payment integrity, payers and cost-containment vendors increasingly use algorithms to detect errors and overpayments. A provider-side audit partner has to keep up with that environment using specialty-specific rules, current payer edits, and exception handling that software alone can't manage.
Questions that separate strong partners from weak ones
Start with operational depth, not sales language. The right questions are practical:
- Do they understand your specialty codes and modifiers? A partner should speak fluently about the claims you bill every day.
- Can they explain payer-specific denial behavior? Generic coding knowledge isn't enough if your major commercial payer has its own edit logic.
- What do their reports change? If the deliverable is just a spreadsheet of errors, you won't get much operational lift.
- How do they work with your existing EHR and staff? A useful audit should fit into your current environment rather than disrupt it.
This checklist of questions to ask a medical billing company before hiring is a solid starting point if you're evaluating outside help.
What to look for in the engagement itself
A capable partner usually shows a few consistent traits:
- Specialty fluency: They know the difference between a coding issue and a workflow issue in your field.
- Transparent methodology: They can explain how they sample, what they review, and how they prioritize claims.
- Actionable reporting: Findings come with recommendations that your team can implement.
- Collaborative posture: They work with providers, managers, and billing staff without creating noise or blame.
The wrong partner focuses on isolated errors. The right partner identifies why those errors keep occurring and how to stop them at scale.
Frequently Asked Questions about Medical Bill Audits
How often should a physician practice run a billing audit
Most practices shouldn't treat auditing as a one-time event. If your payer mix, providers, locations, or service lines are changing, routine review makes more sense than waiting for a major revenue problem. High-complexity specialties usually need more frequent oversight than low-variation practices.
Will an audit only find compliance problems or can it recover revenue too
It should do both. A weak audit points out risk and stops there. A strong audit finds underpayments, missed charges, documentation gaps affecting reimbursement, and payer-specific patterns that can be appealed or prevented going forward.
What records should we expect to provide
Expect to provide chart notes, charge tickets or encounter data, claim data, remittance details, denial reports, payer correspondence, and access to policy or contract details where available. The more complete the data set, the more useful the findings will be.
Can we audit our current billing company without replacing them
Yes. In many cases, that's the smartest first move. An independent audit can clarify whether the issue is staffing, coding, payer follow-up, front-end intake, provider documentation, or the billing vendor's execution. You don't need to change vendors before you understand the root cause.
If you want an outside view of where revenue is leaking in your practice, Happy Billing can help. You can request a free billing audit review or explore specialty-focused support for groups like anesthesiology, cardiology, orthopedics, mental health, pediatrics, and more.