Medical Billing Clearinghouse Services a Practice Guide
A medical billing clearinghouse is the digital intermediary that translates and routes your claims to payers, and for practices under 150 claims per month, a standalone clearinghouse can become a financial drag when per-claim fees run $0.50 to $1.50. More important, 40% of denial root causes happen after format validation, which means a claim can look clean in the clearinghouse and still hurt your cash flow.
That's the trap. Physicians hear “clean claim submission” and assume the revenue problem is solved. It isn't. A clearinghouse helps reduce front-end rejections and can shorten the path from submission to payment, but it does not fix missing authorizations, specialty-specific modifier errors, global period conflicts, or payer policy mismatches. If your denial rate stays stubborn while your clearinghouse dashboard looks fine, you're probably dealing with false clean claims.
For an owner, this is not a technical distinction. It's a margin issue. Every claim that passes the scrubber but dies at the payer adds avoidable work, stretches A/R, and forces your team to chase money you should have collected the first time.
What Are Medical Billing Clearinghouse Services
A medical billing clearinghouse service is the electronic middle layer between your practice and the insurance payer. Under HIPAA, clearinghouses are a recognized intermediary category and the only covered entity permitted to translate between standard and non-standard transaction formats, which is why they're foundational to electronic claims submission in U.S. healthcare, not just another add-on tool (HRSA explanation of healthcare clearinghouses).
If your EHR or PM system creates claim data in one format and the payer expects the HIPAA 837 transaction, the clearinghouse handles that translation and sends the claim to the right destination. That alone matters because it cuts down on manual portal work and standardizes billing across many fragmented payers.
What the clearinghouse actually does
At a practical level, most medical billing clearinghouse services handle four jobs:
- Format translation: They convert claim data into the payer-ready electronic format.
- Basic validation: They check whether core fields are present and structurally valid.
- Routing: They send the claim to the correct payer or network.
- Early response handling: They return initial acknowledgments, rejections, status messages, and often ERAs.
That's useful. It's also incomplete.
A clearinghouse is best understood as a translation and routing layer, not a full denial-prevention strategy.
Where owners get misled
The danger starts when practices confuse clearinghouse acceptance with payer payment. Those are not the same event.
A claim can pass the clearinghouse because the demographics are present, the NPI is valid, and the CPT and diagnosis codes are formatted correctly. Then the payer rejects or denies it because the patient's coverage changed, the authorization lapsed, the modifier logic doesn't fit the specialty scenario, or the service sits inside a global period.
That gap is where owners lose money while thinking the system is working.
If you want the larger context, this is really a revenue cycle design issue, not just a claim-transmission issue. Our view aligns with the broader framework explained in this revenue cycle management overview. The clearinghouse sits in the middle of the process. It does not control the whole process.
My recommendation
If you own an independent practice, treat the clearinghouse as necessary infrastructure, not as proof that your RCM is healthy. It should make submissions cleaner and faster. It should not be the only thing standing between your claims and denial.
That distinction matters most in anesthesiology, behavioral health, orthopedics, cardiology, pain management, and any practice where payer logic is more complex than a basic office visit.
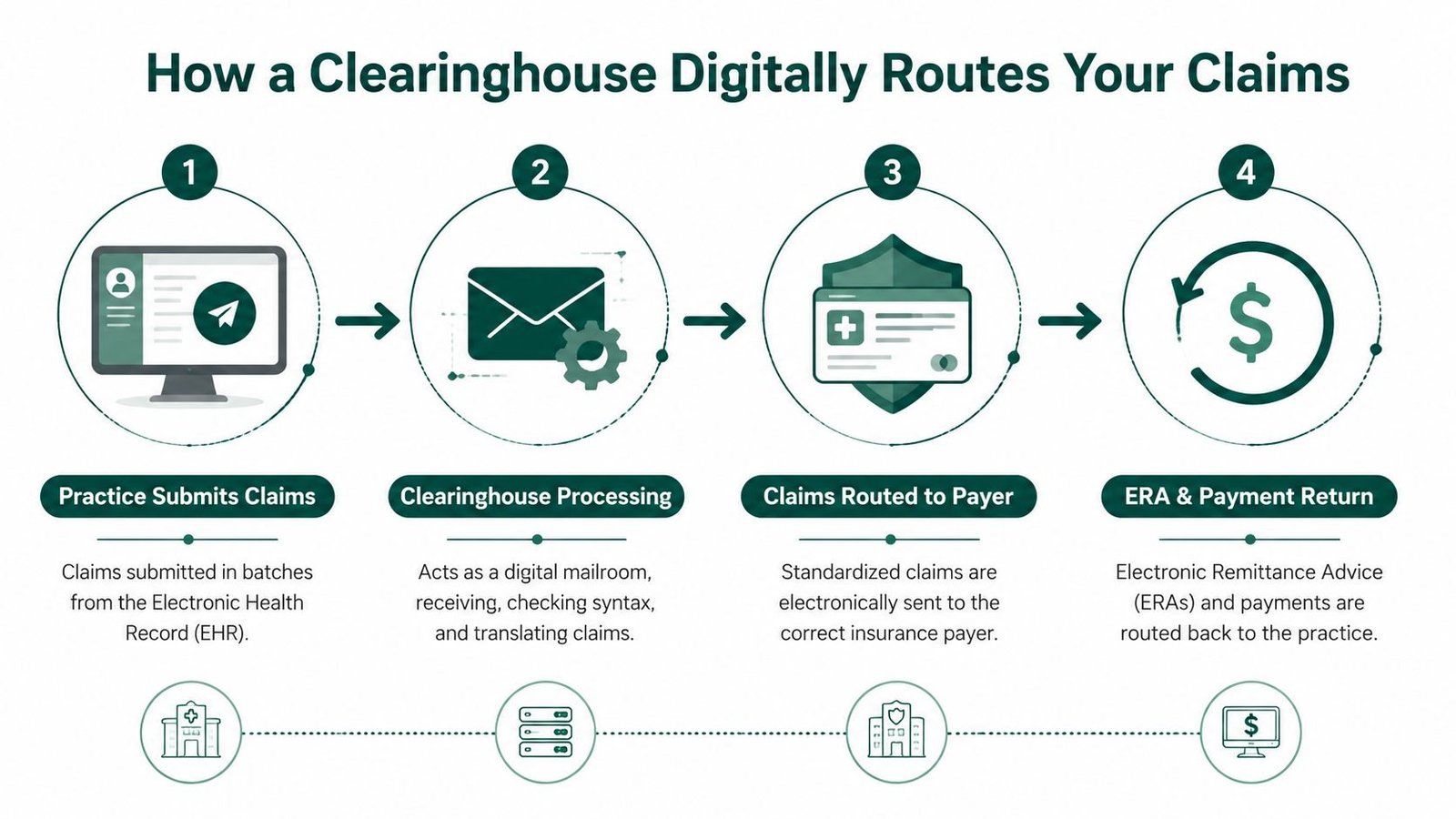
How a Clearinghouse Digitally Routes Your Claims
Think of the clearinghouse as your practice's digital mailroom. Your system sends out one batch. The clearinghouse sorts it, translates it, and directs each claim to the right payer without forcing your staff to log into multiple payer portals.
The basic routing sequence
Here's the working flow inside most clearinghouse setups:
- Your practice submits claim batches from the EHR or PM system.
- The clearinghouse receives the file and checks whether the data is readable and complete enough to process.
- It translates the claim into the HIPAA-required 837 format when needed.
- It routes each claim to the appropriate payer.
- It receives responses back such as acknowledgments, rejections, claim status information, and often ERA files for the practice.
This is why clearinghouses remain so central. A fragmented payer market becomes manageable only when one system standardizes the outbound and inbound traffic.
Why this matters operationally
Without that routing layer, your staff ends up doing more manual work, more portal switching, and more follow-up just to confirm whether a claim got where it needed to go.
The better systems also give you one place to review claim movement rather than scattering visibility across payer websites. That matters for owner oversight. If cash is slowing down, you need to know whether the bottleneck is happening before payer receipt or after adjudication.
For practices reviewing their tech stack, I'd also look closely at how the clearinghouse fits into the rest of your billing infrastructure. This guide on technology for revenue cycle performance is a useful lens for that evaluation.
Don't ignore the file-handling risk
A clearinghouse is moving protected health information constantly. If your workflow still depends on exports, manual uploads, or file transfers between vendors, your operational security matters almost as much as your denial controls. Practices that still move remits, reports, or exception files manually should review basic standards for compliant document handling for businesses and clean up weak handoff points.
When claims move smoothly but documents move badly, payment delays show up later in reconciliation.
My recommendation
Ask a simple question: does your clearinghouse only transmit claims, or does it give your team usable visibility into what happened after transmission?
If the answer is “we send the batch and then someone checks portals later,” you don't have a routing solution. You have a handoff problem.
The Power of Claim Scrubbing for First-Pass Acceptance
The strongest feature in medical billing clearinghouse services is claim scrubbing, the process by which the clearinghouse earns its keep.
According to the HIPAA Journal's overview of clearinghouses, the core value lies in claim scrubbing and standards translation, with validation of patient demographics, insurance data, diagnosis and procedure codes, and related core fields before transmission. That matters because the clearinghouse catches errors in minutes that would otherwise take weeks to come back through adjudication (HIPAA Journal on claim scrubbing and clearinghouses).

What scrubbers catch well
A solid scrubber is good at catching technical defects such as:
- Demographic mismatches: wrong DOB, invalid member ID structure, name discrepancies
- Provider data issues: inactive or invalid NPI, taxonomy problems, missing rendering details
- Code validity problems: nonexistent CPT or diagnosis codes, date mismatches
- Modifier and field omissions: claims missing required supporting data
- Payer edit failures: basic rule conflicts that trigger immediate rejections
If your office bills CPT 99213, 93000, or 20610, a scrubber can help stop obvious problems before those claims ever hit payer intake. If your claim is missing the rendering provider or the insurance ID format is wrong, the clearinghouse should catch it before the payer does.
Why owners should care
Every front-end rejection your team avoids is time saved and cash accelerated. A typo caught today is not a denial appeal next month.
This is the part of the revenue cycle where automation works exactly the way owners want it to. It cuts manual rework. It keeps staff from wasting time on preventable resubmissions. It improves the odds that a claim at least enters adjudication instead of bouncing immediately.
If you want a clean operational definition, this breakdown of what counts as a clean claim in medical billing is worth reading closely.
My recommendation
Use claim scrubbing aggressively, but define success correctly. Don't ask whether the scrubber reduced rejections. Ask whether the scrubber reduced total downstream denials and shortened payment time.
Practical rule: A scrubber should be your first filter, not your only filter.
That mindset change alone helps owners spot why “accepted” claims still fail to produce cash.
The Hidden Ceiling of Standard Clearinghouse Services
Most clearinghouse discussions often become too polite. Standard clearinghouse services hit a ceiling fast, especially in specialty practices.
A 2025 analysis found that 35% of “clean” claims rejected by payers came from specialty-specific logic errors that generic scrubbers failed to flag. In those specialties, the true first-pass clean claim rate fell to 70% to 75%, even though the claims had already cleared front-end checks.

The false clean claim problem
A false clean claim is simple. The claim is technically valid, but operationally wrong.
The clearinghouse sees a formatted claim. The payer sees a denial.
Common examples:
| Specialty area | Claim may pass clearinghouse | Payer still denies because |
|---|---|---|
| Anesthesiology | Modifier QK is valid | concurrency logic doesn't match the documented supervision pattern |
| Behavioral health | CPT and diagnosis pair correctly | authorization requirement or timing rule wasn't met |
| Orthopedics | CPT 27447 is valid | service conflicts with a prior surgery's global period |
| Pain management | Injection code and modifier are present | payer-specific edit or authorization sequence is wrong |
A standard scrubber can tell you a modifier exists. It usually cannot tell you whether the modifier is true for that encounter.
Why generic scrubbing breaks in specialty care
The more your revenue depends on nuanced rules, the less you can rely on syntax-only edits.
In anesthesiology, concurrency is the obvious example. Modifier logic like QK, QX, or AD isn't just a field-entry question. It's a scheduling, documentation, and payer-rule question.
In orthopedic billing, global periods create the same problem. A claim can be perfectly formatted and still fail because the payer views the later service as included in prior surgery.
In behavioral health, a missing authorization isn't a formatting error. It's a workflow failure upstream. The clearinghouse won't rescue you from it.
If your specialty relies on time, sequencing, prior authorization, or episode-of-care logic, a generic scrubber will miss revenue-threatening errors.
My recommendation
Don't judge a clearinghouse by how many claims it accepts. Judge your revenue cycle by the claims that get paid without rework.
If you own a specialty practice and your team is still seeing denials after “successful submission,” assume the problem is not the transmission layer. It's specialty logic.
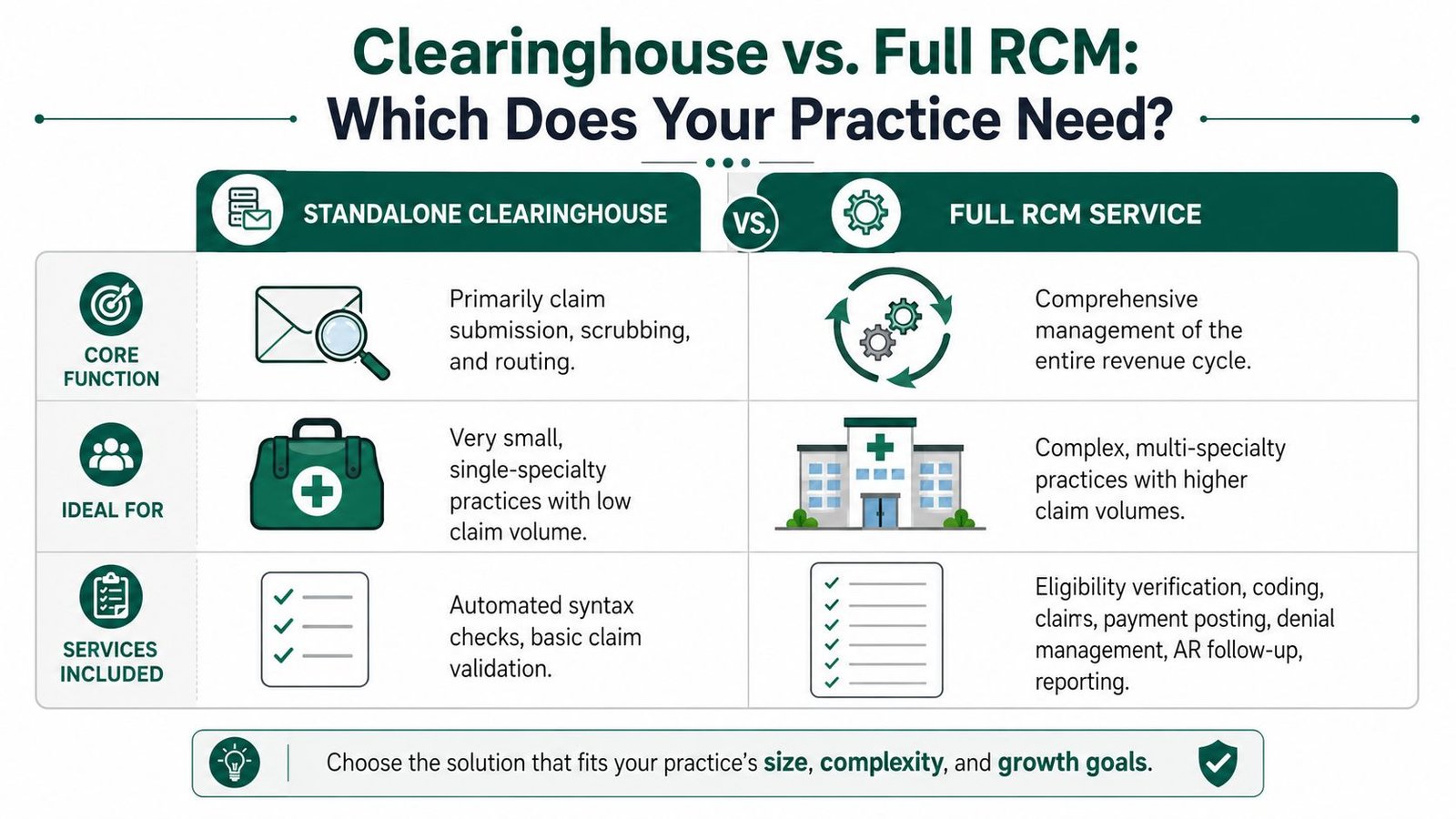
Clearinghouse vs Full RCM Which Does Your Practice Need
Most owners ask the wrong question. They ask, “Do I need a clearinghouse?” You do. The key question is whether a standalone clearinghouse is enough for your practice.
For some practices, yes. For many, no.
The economics matter. For practices with under 150 claims per month, standalone clearinghouse fees of $0.50 to $1.50 per claim can become a liability. That value erodes further because 40% of denial root causes occur after the clearinghouse validates the claim format, including coverage changes and missing authorizations.
When a standalone clearinghouse is enough
A basic setup can work if all of this is true:
- Low complexity: mainly straightforward professional claims
- Limited payer mix: fewer payer rules to manage
- Low claim volume: the owner or staff can still monitor exceptions manually
- Minimal specialty logic: not much reliance on time-based billing, prior auth sequencing, or post-op rules
In that environment, the clearinghouse does what it should. It cleans up clerical mistakes and routes claims efficiently.
When it stops being enough
A standalone clearinghouse becomes the wrong tool when your claims depend on rules outside the claim form itself.
That usually includes:
- Anesthesiology: concurrency, units, and modifier logic
- Orthopedics: global periods and multiple-procedure reductions
- Behavioral health: authorization timing and payer-specific visit controls
- Cardiology and pain management: procedural combinations, medical necessity edits, and payer nuance
If that sounds like your practice, compare your options through the lens of in-house vs outsourced medical billing. Owners often discover they're paying for a transmission utility while still absorbing the labor cost of denial cleanup.
My recommendation
Choose based on claim complexity, not convenience.
If your claims are simple and your payer mix is narrow, a standalone clearinghouse may be enough. If your revenue depends on specialty logic, you need full RCM controls around the clearinghouse. That means eligibility discipline, authorization management, coding review, denial prevention, ERA reconciliation, and active A/R follow-up.
A standalone clearinghouse handles the envelope. Full RCM protects the money inside it.
A Vendor Selection Checklist for Practice Owners
If you're evaluating medical billing clearinghouse services, don't start with price. Start with the leak points in your current revenue cycle.
The U.S. medical billing services market includes 1,364 businesses in 2024, with industry revenue estimated at $4.8 billion by the end of 2024, and IBISWorld projects market size of $4.3 billion in 2026. That's a large, established market, not a niche software category. The same industry view also notes that billing errors cost the U.S. healthcare system over $140 billion annually, which is why front-end validation and downstream control matter so much (IBISWorld overview of the medical billing services market).
The questions that actually matter
Use this checklist before you sign anything:
- Payer connectivity: Ask for the actual payer list that matches your book of business. Don't accept broad marketing language.
- Claim status visibility: Confirm whether you can track payer acknowledgments and not just clearinghouse receipt.
- ERA workflow: Ask how remittance files return and how they're matched for payment posting.
- Rejection handling: Find out whether the system creates action items or just dumps exception reports on your team.
- Enrollment support: Ask who handles payer enrollments and issue resolution during setup.
- Specialty edits: Demand examples of rules relevant to your specialty. For anesthesia, ask about concurrency-related review. For orthopedics, ask about global period conflict checks. For behavioral health, ask about authorization-dependent workflows.
Red flags I would not ignore
Here are the answers that should make you pause:
| Red flag | Why it matters |
|---|---|
| “Our scrubber catches almost everything” | It usually means syntax checks, not specialty logic |
| “We integrate with most payers” | “Most” is useless if your top plans need manual workarounds |
| “Your team can review denials in reports” | That pushes labor back onto your office |
| “Authorization is outside our scope” | Then false clean claims will keep slipping through |
| “We're cheaper per claim” | Cheap transmission doesn't offset expensive denials |
The right vendor reduces rework for your staff. The wrong vendor gives your staff a better-looking queue of unpaid claims.
My recommendation
Walk into vendor meetings with your own denial examples. Use real scenarios. Ask how they'd catch an anesthesia concurrency mismatch, a behavioral health authorization lapse, or an orthopedic post-op billing conflict before submission.
If they answer with generic scrubber language, keep looking.
A stronger evaluation framework lives in these questions to ask a medical billing company before hiring. It's the right checklist if you're trying to protect collections instead of just replacing a vendor.
Frequently Asked Questions From Practice Owners
Is my EHR's built-in clearinghouse good enough
Sometimes, but usually only for simple billing. Built-in clearinghouses are convenient because they reduce one integration point. The tradeoff is that they're often basic. If your practice has specialty-specific denials, prior authorization exposure, or complicated payer rules, convenience won't save you.
What is a reasonable price for clearinghouse services
For practices under 150 claims per month, standalone clearinghouse pricing of $0.50 to $1.50 per claim can erase the value quickly if you still have to do manual denial cleanup. Price only matters after you understand what the service prevents. A cheaper clearinghouse that misses revenue-critical logic errors is expensive in practice.
Should I choose a clearinghouse or full RCM
Choose based on claim complexity. If your claims are straightforward and your payer mix is limited, a clearinghouse may be enough. If you bill anesthesia, orthopedics, behavioral health, cardiology, or pain management, the safer choice is full RCM around the clearinghouse because that's where specialty denials get prevented.
How do I know if I have a false clean claim problem
Look for this pattern. The clearinghouse accepts claims, but denials keep showing up for authorization, medical necessity, modifier logic, global periods, or coverage issues. That means your front-end formatting is working while your revenue controls are not.
If your practice is tired of “accepted” claims turning into unpaid work, Happy Billing is built for exactly that gap. We help specialty practices fix the false clean claim problem with specialty-aware RCM, and you can start with a free revenue cycle audit or review our specialty workflows for groups like anesthesiology practices.