Medical Billing and Practice Management Services: 2026 Guide
If you're looking at medical billing and practice management services in 2026, the direct answer is simple: they matter because they determine how fast your practice gets paid, how much revenue you keep, and how much staff time gets burned on preventable rework. For an independent practice, weak billing operations don't stay in the back office. They show up as rising denials, slower cash flow, and A/R that keeps aging while physicians are still seeing a full schedule.
Most owners come to this question when something already feels off. Collections look inconsistent. Staff says claims are going out. The EHR is full of activity. But bank deposits don't match production, and nobody can explain exactly where revenue is leaking. That's the point where medical billing and practice management stop being an administrative topic and become a financial control system.
What Are Medical Billing and Practice Management Services
Medical billing and practice management services are the operational systems that move a patient encounter from scheduling to payment. In a healthy practice, they connect registration, eligibility, charge capture, coding, claim submission, payment posting, denial follow-up, and reporting into one accountable process.
That definition is too small for most owners, though. In practice, these services are your revenue engine. If front-desk data is wrong, claims delay. If documentation and coding don't line up, reimbursement drops. If follow-up is weak, your A/R stretches and cash gets trapped in receivables instead of funding payroll, hiring, or physician compensation.
The market has grown because practices now treat billing as a strategic function, not an afterthought. The global medical billing market was valued at US$16.8 billion in 2024 and is projected to reach US$27.7 billion by 2029 at a 10.5% CAGR, reflecting how strongly practices are prioritizing cleaner claims, tighter A/R control, and stronger revenue performance according to MarketsandMarkets' medical billing market analysis.
What owners usually miss
Many physicians think billing problems start with coders or collectors. They usually start earlier.
- Front-end failures: bad demographics, inactive insurance, wrong ordering provider, or missing authorization.
- Mid-cycle leakage: unbilled encounters, missed modifiers, incorrect place of service, and delayed charge entry.
- Back-end stagnation: denials sit too long, underpayments aren't escalated, and secondary claims never move.
Practical rule: If your practice can't explain its denial patterns and aged A/R by payer, provider, and location, you're not managing billing. You're reacting to it.
A strong RCM program isn't just software. It's workflow discipline, payer rule awareness, and financial reporting that tells you where cash slows down. If you need a deeper primer on how these pieces connect, this overview of revenue cycle management fundamentals is a useful starting point.
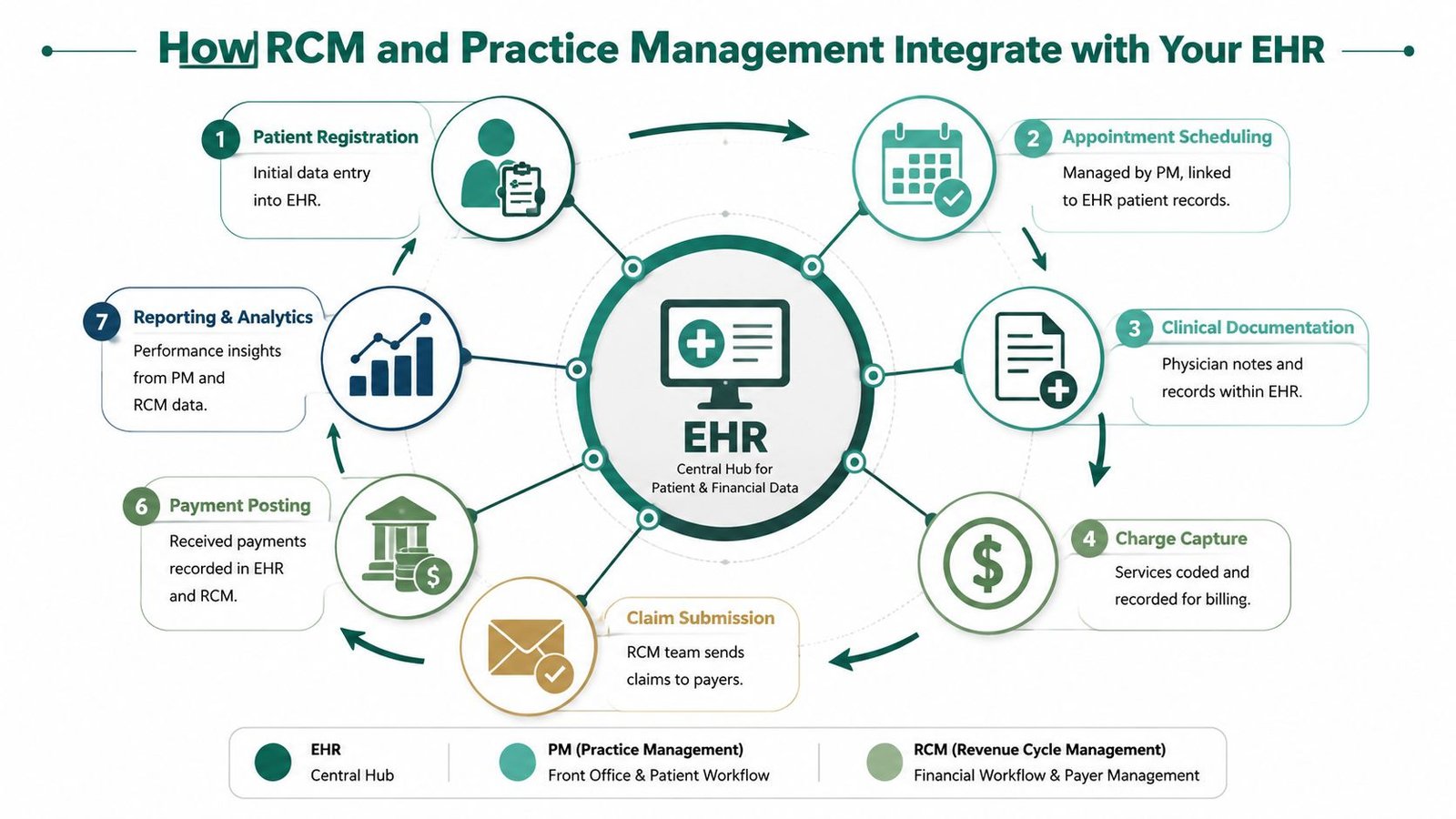
How RCM and Practice Management Integrate with Your EHR
Your EHR, practice management system, and RCM workflow function like a digital nervous system. If information moves cleanly from one point to the next, the practice stays responsive. If signals break, revenue drops before anyone notices.
The costly part isn't usually a dramatic software failure. It's friction. A registration error at check-in becomes a rejected claim. An unsigned note stalls charge release. A scheduling shortcut creates authorization gaps. By the time the problem reaches billing, your staff is already reworking something that should have been correct the first time.
Where integration actually affects money
Owners usually ask whether an outsourced partner can "work with our EHR." That's the right question, but it's too broad. The better question is whether the billing team can operate inside your current workflow without forcing your staff into duplicate entry, shadow spreadsheets, or a migration that disrupts patient flow.
We look for a few specific integration points:
- Scheduling to eligibility: appointments should trigger insurance verification and alert staff before the visit, not after the denial.
- Documentation to charge capture: physician notes, superbills, and procedure logs should release charges quickly and consistently.
- Claim status back to the record: denials, edits, and payer responses should return to a visible work queue, not live in someone's inbox.
- Payment posting to reporting: posted payments should feed financial dashboards that let owners see payer behavior and staff performance.
A practice that's also focused on growth should think about operations more broadly. Front-end scheduling quality affects both access and downstream billing, which is why tools aimed at improving patient acquisition and efficiency can matter financially even before a claim is created.
What works and what doesn't
What works is a partner that uses your existing EHR and PM environment, maps responsibility clearly, and closes handoff gaps. What doesn't work is bolting on another vendor that promises visibility but creates a second source of truth.
When RCM lives outside the EHR with weak reconciliation, practices lose time chasing answers instead of fixing root causes.
We've seen the cleanest transitions happen when the billing team adapts to the practice's current systems rather than forcing a platform change first. That's especially important for physician groups that already have templates, scheduling rules, and documentation habits built into the EHR. If you're evaluating that handoff closely, this guide to integrating revenue cycle management lays out the operational considerations.
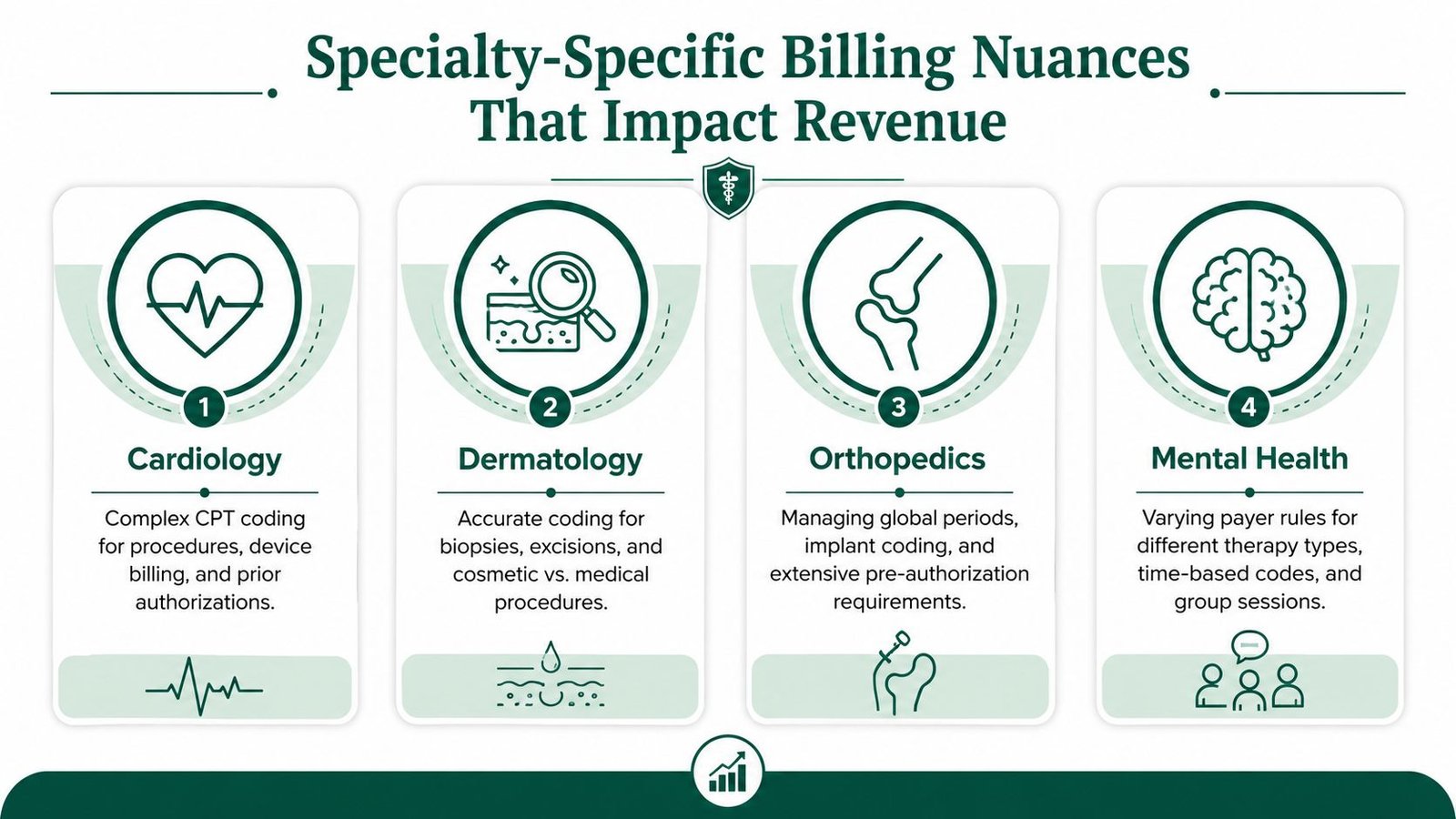
Specialty-Specific Billing Nuances That Impact Revenue
Generic billing support fails when specialty rules start driving reimbursement. That's where most independent practices lose money without realizing it. The claim may go out, but if specialty logic isn't applied correctly, payment comes back reduced, delayed, or denied.
Anesthesiology
Anesthesiology revenue turns on unit accuracy, time capture, and modifier use. If a team mishandles medical direction modifiers such as QK, or fails to reconcile concurrency against the record, the practice doesn't just face a coding issue. It risks being paid incorrectly for high-value cases.
The financial damage often starts with operational sloppiness. An anesthesia record closes late. Time documentation isn't reviewed against the claim. A modifier gets applied by habit instead of by case facts. Those errors don't always look dramatic on a single remittance, but they compound quickly across a busy OR schedule.
Cardiology
Cardiology groups run into a different problem. Many claims are technically submitted correctly but still underperform because procedure coding, component billing, and payer edits weren't reviewed with specialty awareness.
Take CPT 93306 for a complete transthoracic echocardiography study. If your team doesn't manage professional and technical billing correctly, including the use of modifier 26 and modifier TC where appropriate, margin gets eroded. The service was delivered. The machine was used. The interpretation was done. But the claim structure determines whether the practice captures what the contract allows.
A cardiology denial isn't always a denial. Sometimes it's a partial payment that nobody audits.
That's why a generic "collections rate" tells owners very little. You need to know whether your billing team catches reduced payments, bundling issues, and payer-specific edits before they become write-offs. Practices comparing specialty support can review options across fields on the Happy Billing specialties page and drill deeper into cardiology revenue cycle management.
Mental health
Mental health revenue depends heavily on authorization control and time-based coding discipline. A recurring psychotherapy code such as CPT 90837 can be clinically appropriate and still become a revenue problem if authorization limits, visit counts, or payer frequency rules aren't tracked proactively.
One missed authorization checkpoint can create a chain of nonpayment. The clinician keeps seeing the patient. Staff assumes coverage remains active. Then claims start denying in batches. By the time someone notices, the practice is deciding whether to appeal, bill the patient, or write the balance off.
What works in behavioral health is a workflow that ties authorization dates, units, and visit utilization directly to scheduling. What doesn't work is treating authorization as a one-time front-desk task.
The Four RCM Metrics Every Practice Owner Must Track
A practice can feel busy, schedule full days, and still miss payroll targets because cash is getting stuck between charge entry and payment posting. We see this during audits all the time. The owner hears that collections are "fine," but no one can show which part of the revenue cycle is slowing down or leaking margin.
That is why every practice owner needs a short dashboard tied to action. Four metrics usually surface the problem faster than a 20-tab report.
The four numbers that matter
| Metric | What it tells you | What a weak number usually means |
|---|---|---|
| First-pass resolution rate | How often claims pay without rework | Front-end registration errors, coding issues, payer edit failures |
| Days in A/R | How long cash remains outstanding after billing | Slow follow-up, delayed posting, unresolved denials |
| Denial rate | How much billed work comes back unpaid or rejected | Eligibility failures, authorization gaps, documentation mismatch |
| Net collection rate | How much allowed revenue the practice actually collects | Underpayments, avoidable write-offs, poor appeal follow-through |
Each metric answers a different financial question. First-pass resolution measures how much rework your team is creating. Days in A/R measures how long revenue is trapped. Denial rate shows how often preventable friction is interrupting payment. Net collection rate shows whether the practice is keeping the dollars it already earned under payer contracts.
The main value comes from reading them together.
If first-pass resolution drops and days in A/R climbs, the issue usually starts before the claim leaves the practice. If denial rate stays flat but net collection rate weakens, we look for underpayment variance, payer posting errors, or staff writing off balances that should have been appealed. Those patterns matter because they point to very different fixes, staffing needs, and vendor expectations.
We often advise owners to compare these RCM metrics against the monthly income statement with a profit and loss analyzer tool. That side-by-side view makes operational problems easier to spot. Charges may be stable while collections soften. Contractual adjustments may spike for one payer. Overhead may hold steady while cash lag stretches two billing cycles longer.
A metric does not solve the problem. It tells you where to audit first.
One more standard matters. Reporting should break results down by payer, provider, and location. Aggregated totals hide poor performance. A strong orthopedic surgeon can mask weak follow-up for a satellite office. One favorable payer contract can hide chronic underpayments from another. This medical billing KPI dashboard checklist shows the level of reporting detail owners should expect in a monthly review.
If your billing partner cannot produce these four metrics with segmentation and month-over-month trend lines, you do not have management visibility. You have a billing summary.
Common Pitfalls and Proactive Denial Prevention
A patient is seen on Tuesday, the claim drops on Wednesday, and cash still does not arrive. The billing team says the claim was submitted clean. Then the EOB comes back with a denial tied to eligibility, authorization, modifier support, or a payer edit no one checked before the visit. The loss did not start in accounts receivable. It started in the workflow.
That is the core mistake many practices make. They treat denials as back-end billing work instead of front-end revenue control. We audit denials by asking one question first: where did the process fail before the claim was sent? That approach changes staffing decisions, edit rules, and accountability.
Three failure points we see repeatedly
Weak eligibility control
Coverage gets verified at new-patient intake but not again before follow-up visits. Plan terms change. Secondary coverage changes. Referral requirements expire. By the time the denial posts, the front desk error is already 30 to 45 days old, and the balance may no longer be collectible from the patient.
Payer-rule blindness
A clearinghouse acceptance is not proof that a payer will pay. Many denials come from rules that sit outside generic claim edits: authorization windows, frequency limits, modifier expectations, place-of-service conflicts, or documentation standards for a specific plan. A billing service that works inside your daily workflow should catch those rules before submission, not after remittance.
Passive denial work
Teams refile claims, correct minor errors, and mark tasks complete without separating preventable denials from unavoidable ones. That keeps staff busy, but it does not improve cash performance. If denial categories are not trended by payer, provider, location, and root cause, the same mistakes repeat every month.
What proactive prevention looks like
- Verify eligibility before each visit. Confirm active coverage, benefit status, coordination of benefits, and referral or authorization requirements close to the date of service.
- Scrub claims against payer-specific rules. Generic edits catch formatting issues. They do not catch the contract and policy details that drive many first-pass denials.
- Code denials to root cause. Route registration problems to front office staff, coding issues to coders, and documentation gaps to the clinical team.
- Track denial aging and rework time. A denial resolved in 7 days has very different cash impact than one that sits untouched for 28 days.
- Close the loop with operations. If one payer repeatedly denies the same service line, the fix belongs in scheduling, intake, authorization, or documentation, not just in AR follow-up.
Modifier use is a good example. A claim with modifier 59 or a component modifier may pass internal review and still fail if the record does not support separate reimbursement under that payer's policy. The coding choice matters. The workflow control matters more. Someone has to confirm that documentation, payer policy, and edit logic match before the claim leaves the system.
Communication failures also contribute to denials and slow rework. When front office staff, billers, and remote teams cannot reach each other quickly, missed authorizations and unresolved registration questions sit longer than they should. For practices reviewing phone systems as part of workflow cleanup, SnapDial's comparison resource is one way to evaluate business VoIP options that support faster handoffs between scheduling, intake, and billing.
A disciplined billing partner should show denial volume, denial dollars, turnaround time, overturn rate, and repeat root causes. We expect that reporting to be specific enough to tell a practice owner whether the problem sits in registration, coding, documentation, or payer follow-up. If a vendor can only report how many claims staff "worked," they are measuring activity. They are not protecting revenue.
Your Vendor Selection Checklist
Choosing a billing vendor isn't a rate-shopping exercise. It's an operating model decision. The wrong partner can preserve all the same leak points you already have, just under a different logo.
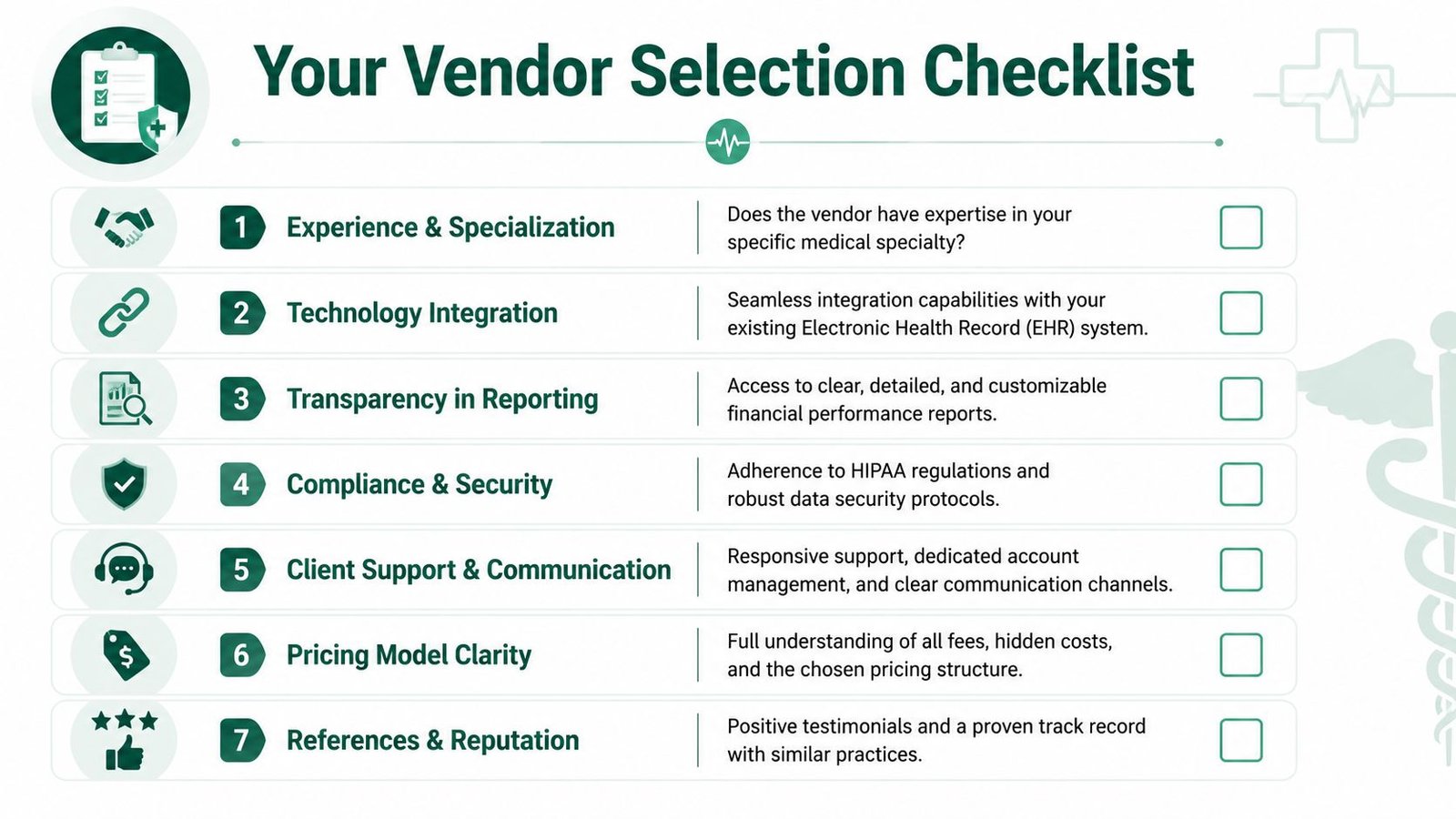
Buyers are often handed generic checklists, but stronger evaluation starts with workflow outcomes. A recent industry guide highlights the importance of asking whether a vendor integrates with your current EHR, offers clear pricing, and can benchmark operational measures such as denial turnaround and claim edits prevented, not just headline collections, as discussed in this medical billing vendor evaluation guide.
The questions that actually expose risk
Ask these in writing and compare answers side by side.
- Will you work inside our current EHR? If the answer is vague, expect disruption, duplicate work, or a long stabilization period.
- How do you handle our specialty's codes and payer rules? A real partner should speak comfortably about your common CPT patterns, modifiers, authorization needs, and denial categories.
- What is included in your fee? Owners should know whether credentialing, patient statements, payment posting, denial appeals, and old A/R follow-up are included or billed separately.
- How do you report performance? Ask for sample dashboards that show denial categories, A/R aging, payer lag, and unresolved claim value.
- Who owns communication? You need named contacts and escalation paths, not a shared inbox.
Compare vendors like an operator
A simple comparison framework helps. If you've ever used SnapDial's comparison resource to evaluate service providers on support, pricing clarity, and operational fit, use the same discipline here. Billing vendors also need to be compared on implementation friction, accountability, and responsiveness, not just price.
A cheap billing fee becomes expensive when your physicians wait longer to get paid.
This is also the section where we tell owners to ask for proof, not promises. Request reporting samples. Ask how quickly denied claims are touched. Ask how they separate preventable denials from clinical denials. Ask how they handle old A/R. If a vendor can't answer those operational questions clearly, their collection percentage won't help you much.
One example in the market is Happy Billing's free revenue cycle audit, which gives practices a structured way to review current denial patterns, workflow gaps, and A/R issues before making a vendor decision. That's the right sequence. Audit first. Contract second.
Calculating ROI and Understanding Pricing Models
Most outsourcing decisions get framed the wrong way. Owners ask, "What percentage do you charge?" The better question is, "What revenue do we recover, how fast, and with what level of visibility?"

The common pricing models
| Model | Usually fits | Main trade-off |
|---|---|---|
| Percentage of collections | Practices that want aligned incentives and flexible support | Cost rises with collections, so reporting transparency matters |
| Flat fee per claim | Stable claim volume and simpler service lines | Can create misalignment if denials and follow-up work vary widely |
| FTE or dedicated staffing model | Larger groups that need embedded workflow coverage | Requires stronger management oversight and clearer scope |
How to think about ROI without fake precision
You don't need invented benchmarks or inflated promises to calculate value. Start with your own baseline.
Review:
- current denial categories
- days in A/R by aging bucket
- underpayment follow-up
- old A/R recovery
- charge lag from date of service to submission
- staff hours spent on rework
Then compare those costs against the vendor fee and the expected operational change. If a billing partner shortens claim submission lag, improves denial handling, and gives you better visibility into underpayments, the financial return comes from recovered revenue and faster cash conversion, not from a marketing promise.
We've found this analysis works best when owners compare pricing model fit against actual workflow complexity. A mental health group with authorization-heavy billing may need a different structure than a cardiology practice with high procedural complexity. If you want a practical breakdown, this guide on medical billing outsourcing cost is useful for framing the decision.
Frequently Asked Questions
Should we outsource billing or fix our in-house team
If the problem is isolated training, a strong in-house team may be worth rebuilding. If the problem includes poor reporting, missed follow-up, specialty billing errors, and weak EHR workflow integration, outsourcing often makes more sense because you're fixing process, staffing, and accountability at the same time.
How long does a billing transition usually disrupt collections
The answer depends on data access, EHR setup, payer enrollment status, and how clean your current workflows are. The least disruptive transitions happen when the new partner works inside your existing systems and takes over responsibilities in a controlled sequence rather than forcing a platform change.
What should we ask for in the contract
Ask for scope, reporting frequency, denial handling responsibilities, communication cadence, old A/R ownership, and termination terms. Also ask how pricing changes if your volume shifts or if additional services are needed.
What performance should we expect from a billing partner
Expect clear reporting, accountable denial follow-up, fast issue escalation, and specialty-aware workflow control. If a partner can't show you where cash is slowing down, they aren't really managing your revenue cycle.
If your practice is dealing with rising denials, slow payments, or unclear billing performance, Happy Billing can help you evaluate the problem at the workflow level instead of guessing. A billing relationship should improve cash flow, reduce rework, and give owners cleaner financial visibility. That's the standard worth using.