Medical Billing Consulting Services: A Guide for Practices
About 30% of insurance claims are denied on first submission, and that's exactly why medical billing consulting services matter. Done right, they function as a strategic diagnostic that finds where your practice is losing cash, fixes the workflow failures behind denials and delays, and helps you protect revenue while shortening A/R.
If you own or run an independent practice, you shouldn't think of billing consulting as “extra help with claims.” You should treat it as a margin-protection tool. In our experience, the question isn't whether your team is working hard. It's whether your current billing process is converting clinical work into cash quickly, accurately, and consistently.
What Are Medical Billing Consulting Services
Medical billing consulting services are not the same as basic outsourced billing. A billing company may submit claims and post payments. A consultant should diagnose why money is getting stuck in the first place.
That distinction matters because physician owners don't lose money only when a claim is left unfiled. They lose money when registration errors trigger avoidable denials, when authorization workflows fail, when coding rules are applied inconsistently, and when old A/R sits untouched until it becomes write-off risk.
The market size alone tells you this isn't a side issue. Fortune Business Insights projects the global medical billing outsourcing market will reach USD 50.47 billion by 2034 with a 12.05% CAGR, and says North America held 55.12% of the market in 2025 in its medical billing outsourcing market analysis. When a market grows at that scale, it usually means practices are under pressure to tighten operations, not just hand off paperwork.
It's a financial diagnostic, not a clerical service
A strong consultant looks at your revenue cycle the way a good specialist reviews a difficult case. They don't stop at the symptom.
They ask:
- Where are denials starting: Front desk, eligibility, authorizations, coding, claim edits, or payer follow-up
- Which workflows leak money: Missed charges, documentation gaps, untimely filing, underused modifiers, weak appeal processes
- What slows cash: A/R aging by payer, by location, by provider, and by service line
Practical rule: If a consultant talks mostly about “taking billing off your plate,” you're talking to an outsourcer. If they talk about root causes, controls, payer trends, and KPI movement, you're talking to a consultant.
For physician owners who want a solid operational baseline, this overview of revenue cycle optimization tips is useful because it reinforces the same reality we see every day. Revenue problems rarely come from one claim. They come from repeated process failures.
Why this matters to practice owners
A mature practice can still bleed cash unnoticed. That's why we push owners to evaluate billing with the same discipline they apply to staffing, scheduling, and payer contracts.
If you're comparing options, start with a practical primer on medical billing services for physicians. Then ask the harder question. Is your current partner just processing work, or are they actively finding and fixing revenue leakage?
Core Offerings of a Billing Consultant
A real consultant performs a full revenue-cycle diagnostic. That means tracing breakdowns across registration, insurance verification, charge capture, coding, claims submission, payment posting, and denial follow-up. That end-to-end approach matters because, as explained in this review of effective medical billing consulting workflows, front-end mistakes create downstream denials, delays, and rework.
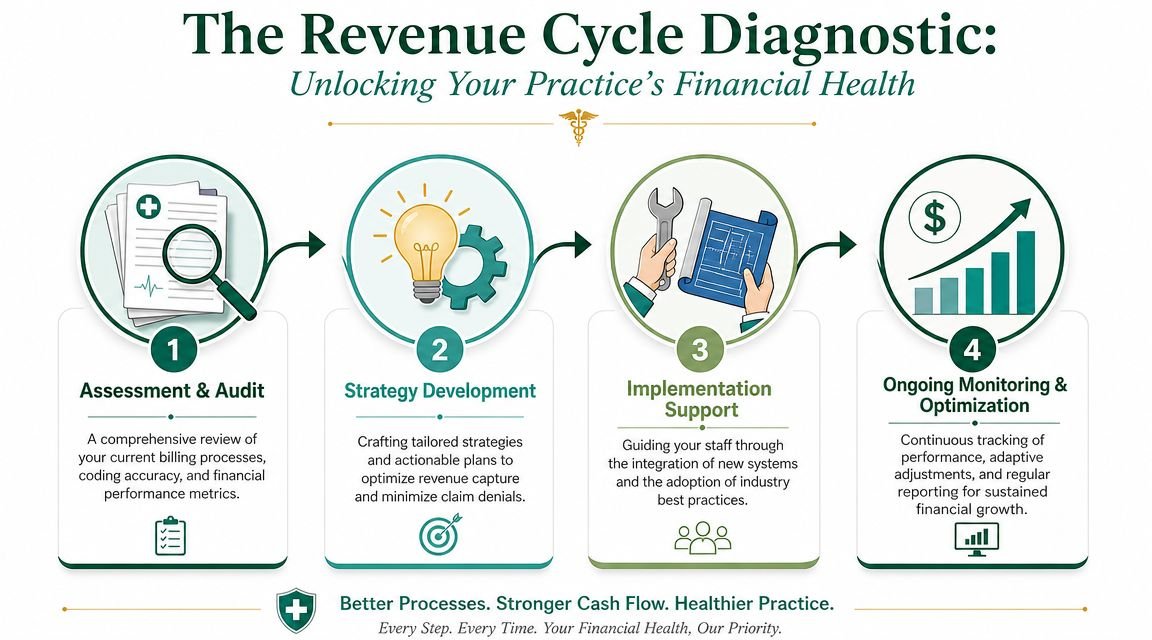
What they should actually review
If a consultant doesn't inspect the full chain, they'll miss the source of the problem. We usually expect a serious engagement to cover these areas:
- Front-end intake controls: Demographics, eligibility, coordination of benefits, and authorization capture
- Charge capture reliability: Whether every billable encounter, procedure, and supply is making it into the claim queue
- Coding and documentation alignment: CPT, HCPCS, diagnosis linkage, modifier use, and documentation support
- Claim production quality: Edits, scrubbing logic, payer-specific rules, and submission timing
- Back-end recovery: Denials, underpayments, appeals, payment variance review, and old A/R follow-up
The best consultants don't just fix denials
They track the denial back to the operational cause.
A registration typo is not a registration problem. It becomes a denial problem, then an A/R problem, then a cash-flow problem, then an owner frustration problem. That's why consulting has to be cross-functional.
We've found that busy practices benefit most when consultants document findings in a way leadership can act on fast. Not fifty pages of theory. A short list of failure points, ownership, deadlines, and expected KPI impact.
The right consultant should be able to tell you which part of your workflow causes the problem, who needs to change behavior, and how success will be measured.
What implementation support should look like
A good consultant stays involved after the audit. Otherwise, the practice learns what's broken and then gets no traction fixing it.
Expect support such as:
- Rule changes inside your PM or EHR so common payer edits stop recurring.
- Targeted staff training for front desk, coding review, or payment posting teams.
- Denial trend analysis that groups recurring issues by payer, provider, location, or service.
- Reporting discipline so leaders can see whether corrections are sticking.
Some practices also benefit from process automation ideas borrowed from other A/R-heavy industries. This article on AR automation for logistics teams isn't healthcare-specific, but it's a useful reminder that disciplined follow-up, routing, and reporting can materially improve collections workflows in any receivables operation.
If your denial backlog is already hurting cash flow, it also helps to review what specialized denial management services should include before you hire anyone.
Why Specialty-Specific Expertise Is Not Negotiable
General billing knowledge isn't enough. A consultant can be competent and still miss revenue in your specialty every week.
That's because the financial risk sits inside specialty rules. If your consultant doesn't understand how your claims are paid, they can't diagnose leakage with any precision.

Anesthesiology, behavioral health, cardiology, orthopedics
Take anesthesiology. If a consultant can't speak comfortably about base units, time units, and modifiers like QK, they're not equipped to assess whether your medical direction model is being billed correctly. Small mistakes there don't just cause denials. They can reduce reimbursement or create compliance exposure.
Behavioral health has a different risk profile. Codes like 90837 depend on session structure, time support, and payer rules. Prior authorization discipline matters. So does making sure the documentation supports the billed service and that telehealth rules are handled correctly when applicable. A consultant who treats mental health like primary care billing will miss both payment delays and preventable write-offs.
Cardiology is another example. Practices often lose money on diagnostic imaging edits, interventional coding complexity, and bundling issues tied to procedural combinations. If your consultant doesn't understand how those claims are edited and paid, “cleaning up billing” becomes generic advice with little financial impact. For cardiology groups specifically, this guide to cardiology medical billing services is a good reality check on the level of specialty detail your partner should be able to discuss.
The owner's test for real expertise
Ask the consultant to walk through claims from your specialty and explain where money is usually lost.
A specialist should be able to discuss examples like:
- Modifier risk in surgery and orthopedics: Global periods, post-op visit confusion, and multiple procedure reductions
- Time-based coding in behavioral health: Whether the billed session length is supported and authorized
- Concurrency and direction in anesthesia: Whether staffing models and modifiers line up with documentation
- Bundling pressure in cardiology: Whether procedural combinations trigger edits or payment reductions
If a consultant answers specialty questions with broad phrases like “our coders know all specialties,” that's not expertise. That's a dodge.
We've seen owners save time and avoid bad-fit vendors by starting with a partner's specialty footprint instead of their sales presentation. If you want to compare by field, browse specialty billing resources and look for evidence that the firm understands your procedure mix, payer behavior, and revenue risks at the claim level.
The Business Impact Measured in Dollars and Days
A few percentage points in collections can decide whether a practice has cash to hire, invest, or cover payroll without stress. That is the standard owners should use when they evaluate a billing consultant.
IBISWorld reports the U.S. medical billing services market was contracting at a 2.2% CAGR from 2019 to 2024 in its medical billing services industry analysis. In our experience, that makes consultant quality more important, not less. Mature markets reward operators who fix bottlenecks, tighten follow-up, and protect margin. They punish vague advice.
The four KPIs that matter most
If a consultant cannot tie their work to these four numbers, keep looking.
| KPI | What it tells you | Why it matters |
|---|---|---|
| First-pass clean claim rate | How many claims go out correctly the first time | Better clean-claim performance gets claims paid faster and cuts staff rework |
| Denial rate | How often payers reject claims initially | Denials increase labor, delay cash, and push more balances into aging |
| Days in A/R | How long claims and balances sit before payment | Lower A/R improves cash flow and reduces the odds that collectible revenue turns into write-offs |
| Net collection rate | How much of allowed revenue the practice actually collects | This is the clearest measure of whether your revenue cycle is keeping earned income |
MGMA notes that many high-performing medical practices target a net collection rate in the mid-to-high 90% range, as outlined in its medical practice financial benchmark guidance. We use 95% to 97% as a practical benchmark for many specialties. If you are below that range, do not accept broad explanations. Find the exact points where allowed dollars are being lost.
How consulting changes those numbers
Good consulting changes cash flow by changing behavior inside the revenue cycle.
Eligibility work cuts preventable front-end denials. Coding and charge capture reviews improve claim accuracy before submission. Follow-up rules, appeal discipline, and payer-specific work queues shorten payment cycles and recover dollars that would otherwise age out.
The point is measurement. We recommend setting a baseline before the engagement starts, then reviewing KPI movement every 30 to 60 days. If denial rate drops but days in A/R stays flat, the follow-up process still has a problem. If clean claims improve but net collections do not, the issue may be underpayments, weak appeals, or avoidable contractual write-offs.
Owner mindset: Ask, “Which KPI moved, by how much, over what time period, and what workflow change caused it?”
If cash is landing too slowly, review this guide to days in A/R and what healthy payment timing looks like with your consultant or billing team. It gives you a direct way to connect operational fixes to days saved and dollars collected.
Understanding Pricing Models and Calculating ROI
Billing consulting fees only matter in relation to the dollars they return. We recommend judging every proposal on one standard: how fast it improves cash, reduces leakage, or lowers avoidable labor.
Most engagements fall into three pricing structures. Percentage-of-collections agreements tie fees to ongoing performance and fit full-scope billing oversight. Per-claim pricing works better in stable, high-volume settings where claim complexity is predictable. Flat monthly fees make sense for audits, workflow redesign, staff training, and management oversight when you are not replacing the billing function.
The wrong move is comparing those models on price alone. Compare them on scope, accountability, and the financial problem you need solved. A 5% arrangement can be cheap if it raises collections and shortens payment cycles. A low flat fee is expensive if it produces a report, a few meetings, and no KPI movement.
Here is the framework we use with physician-owners.
First, define the baseline. Pull your last 90 to 180 days of net collections, denial rate, first-pass resolution, days in A/R, and aged A/R over 90 days. Then identify the leak that matters most. Front-end eligibility failures, coding misses, weak denial follow-up, and payer underpayments do not produce the same ROI profile, so they should not be priced or judged the same way.
Second, match the fee model to the job.
- Percentage of collections: Best for ongoing execution where the consultant influences daily billing output and follow-up discipline.
- Per-claim pricing: Best for standardized claim production with limited consulting depth.
- Flat monthly consulting fee: Best for diagnosis, training, process repair, and leadership oversight.
Third, calculate ROI in dollars, not impressions. Use a simple formula: additional monthly cash collected plus labor savings, minus consulting cost. If a consultant helps recover missed revenue, reduces rework for your staff, or cuts aging enough to improve cash timing, the engagement is paying for itself.
A quick example makes this practical. If a practice collects an extra $25,000 per month after denial cleanup and payer follow-up improvements, and the consulting fee is $8,000, the gross monthly return is $17,000 before any added labor savings. That is the kind of math owners should demand.
For owners comparing options, this breakdown of outsource medical billing cost is useful because it separates transaction pricing from true consulting economics.
One more point gets missed. Operational dependencies affect ROI. If your front desk cannot verify coverage, or your phones create scheduling and registration gaps, your billing consultant will spend time cleaning up preventable errors. We see the same issue in adjacent vendors such as choosing the right answering service partner. Upstream workflow quality changes downstream collections.
Our recommendation is simple. Do not ask, “What do you charge?” Ask, “Which KPI will you move first, by how much, and how will that change monthly cash?” That question filters out generic firms fast.
How to Evaluate a Consulting Partner
Most firms sound good in a proposal. Very few can explain exactly how they'll diagnose your revenue cycle, prove impact, and work inside the realities of your specialty and software.
That's the problem with generic marketing in this category. The more a firm talks about being “customized” and “error-free,” the more carefully you should interrogate their process. A key differentiator is whether they can define their audit scope, benchmark method, and internal-control review, as outlined in this medical billing consulting overview.
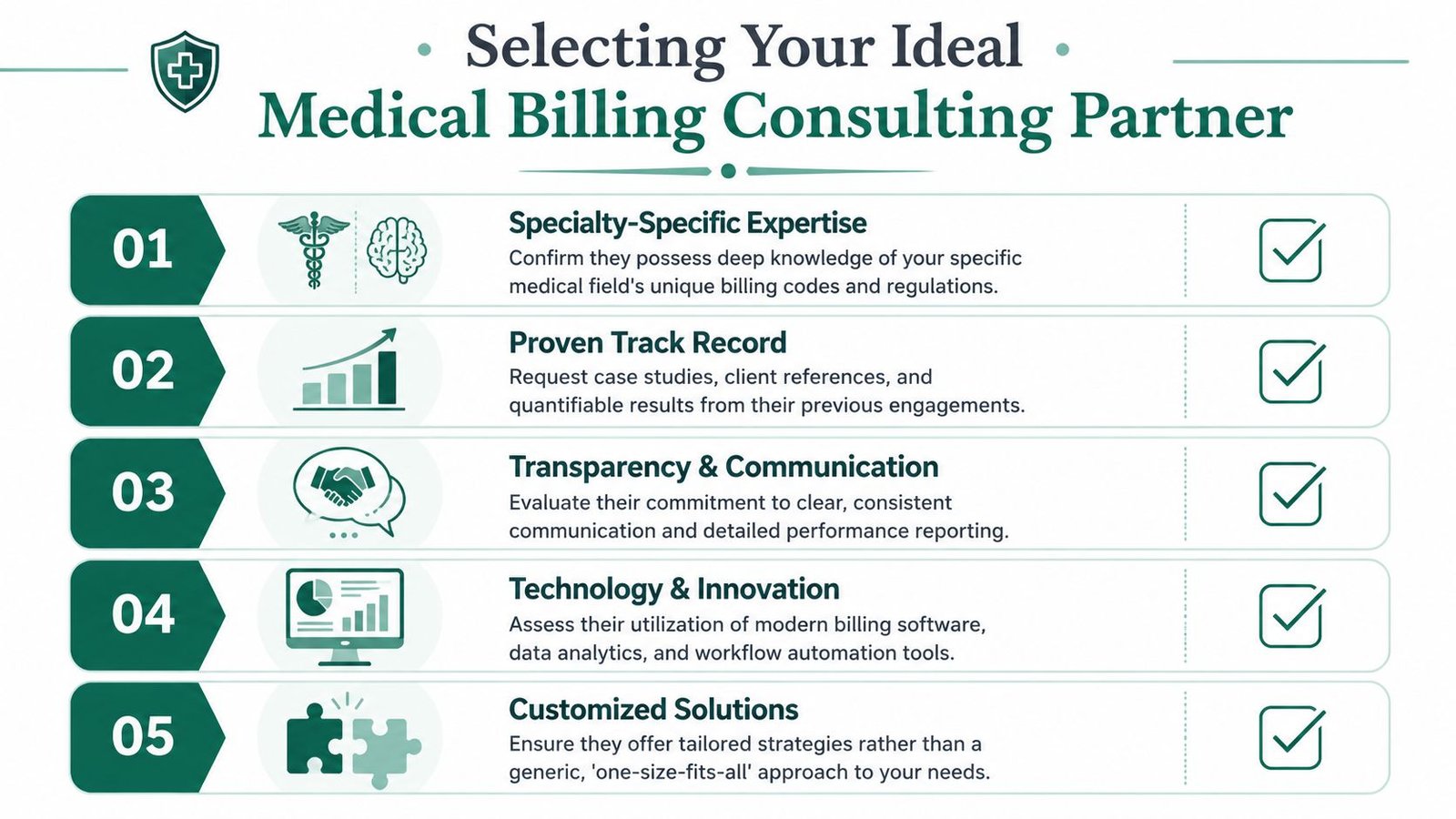
The questions worth asking
Ask these in the first meeting, not after the contract arrives:
- What exactly do you audit: Registration, eligibility, coding, claims edits, payment posting, denials, A/R aging, underpayments, and payer mix should all be on the table.
- How do you benchmark performance: If they can't explain how they judge your clean claims, denials, net collections, or A/R, they can't prove progress.
- How do you test internal controls: You want to know how they identify repeatable process failures, not just isolated mistakes.
- Can you work inside our current EHR and PM setup: Forced migrations create friction and often delay results.
- How do you report impact to leadership: Busy owners need clear reporting, not jargon.
One company that fits the “works inside your existing EHR” model is Happy Billing, which positions its service around full-cycle RCM, denial management, specialty workflows, and operating without a system migration. That operating model can be practical for owners who want workflow improvement without a software overhaul.
Red flags you shouldn't ignore
Bad partners reveal themselves early.
- Vague language: They promise support but can't describe process diagnosis.
- No specialty depth: They avoid specifics when you ask about your CPT mix, modifiers, or payer habits.
- Weak reporting: They talk about effort, not outcomes.
- Rigid systems: They want you to adapt to their workflow instead of fitting into yours.
- Contract-first behavior: They push signatures before they've reviewed your data.
A consultant should earn trust by showing how they think, not by asking you to trust the sales pitch.
This article on choosing the right answering service partner comes from a different service category, but the buying logic is similar. Process transparency, fit, accountability, and reporting matter more than polished claims.
Frequently Asked Questions
Should I hire a consultant if I already have an in-house biller
Yes, if you suspect hidden leakage or stagnant A/R. A consultant and an in-house biller do different jobs. Your biller executes the day-to-day work. A consultant should examine the system, identify failure points, and redesign weak processes so your internal team can perform better.
What's the difference between outsourced billing and consulting
Outsourced billing handles production tasks such as claim submission, payment posting, and follow-up. Consulting focuses on diagnosis, controls, workflow design, staff training, payer-pattern analysis, and KPI improvement. Some firms do both, but you should confirm which one you're buying.
How do I know if my current billing partner is underperforming
Look at operational symptoms. Cash is slow. Denials repeat. Leadership reporting is vague. Old A/R keeps growing. Specialty-specific issues keep coming back. If your partner can't explain the root cause behind those patterns and show you what they changed, they're probably maintaining problems instead of solving them.
What should I ask for before signing an agreement
Ask for a defined audit scope, reporting examples, specialty experience, EHR compatibility, ownership of workstreams, and the KPIs they'll use to judge success. Also ask how they'll handle payer-specific problems, coding audits, denial trends, and whether they can show findings in a way a physician-owner can act on quickly.
If your practice is dealing with rising denials, slow cash, or billing that feels busy but not effective, the next step is simple. Talk with Happy Billing and start with a focused review of where revenue is leaking, which workflows are causing it, and what changes will improve collections and A/R.