IDR Process No Surprises Act: Win Disputes & Protect Revenue
If you're dealing with out-of-network payments under the No Surprises Act, the IDR process isn't just a compliance task. It's a revenue decision. Handle it well and you can recover underpaid claims that would otherwise sit in A/R or get written off as payer friction.
Most practice owners run into the same problem. A payer sends a payment that doesn't reflect the acuity, setting, or physician expertise involved in the case. Your team knows the amount is weak, but the next step feels technical, deadline-driven, and easy to lose on procedure alone. That's exactly why the IDR process under the No Surprises Act matters to practice owners. It directly affects cash flow, denial recovery, and how much advantage you have when a plan underpays a protected out-of-network claim.
Winning Surprise Billing Disputes Starts Here
Monday morning. Your team posts an ERA for an out-of-network emergency claim, and the payment is far below any reasonable commercial rate for the work performed. The patient is protected from balance billing, so the shortfall lands on the practice unless someone acts fast and documents the case well enough to challenge the payer's number.
That is the financial reality behind the No Surprises Act. For physician groups, the law created a formal payment dispute path for certain out-of-network claims instead of a dead end. The opportunity is real, but so is the risk. A weak IDR process turns valid underpayments into write-offs, stale A/R, or payer precedent that drags down future reimbursements on similar cases.
We see the same operational mistake across hospital-based specialties. Leadership treats IDR as a legal or compliance task, then hands it off too late with thin documentation and no claim selection discipline. Payers benefit from that hesitation. They know many practices will miss deadlines, skip smaller but still material claims, or file with generic arguments that do not explain acuity, setting, physician training, call coverage obligations, or the actual market value of the service.
The groups that recover more money approach IDR as a revenue channel with rules, economics, and repeatable tactics. Anesthesiology disputes often rise or fall on time units, physical status support, concurrency records, and coverage expectations. Cardiology and other hospital-based procedural specialties often need a tighter story around emergent decision-making, physician availability, and why the payer's offer fails to reflect the service delivered. Orthopedic and trauma claims can justify the effort quickly because one underpaid case can distort the month.
If you need a grounded refresher on the operational side of protected claims, this guide to surprise billing rules and workflows lays out the core intake and follow-up issues.
Where practices actually lose margin
Losses usually start before the IDR filing itself. The claim is not screened early. Open negotiation is started late or with weak support. The submission package repeats the billed charge and says little about why the payer's amount is inadequate. Then the practice decides arbitration is not worth the trouble.
The better conclusion is narrower. Poorly prepared disputes are not worth the trouble. Well-chosen, well-supported disputes often are.
That distinction matters because payers are not passive participants. They contest eligibility, force provider groups to prove basic facts already present in the record, and anchor low offers in the hope that the practice will decide the administrative work is too expensive. Winning starts with selecting disputes that justify the effort and building an evidence file that answers the payer's likely objections before they raise them.
A similar discipline shows up in other regulated operating environments. Teams that perform well under pressure use defined intake rules, documentation standards, and escalation controls instead of relying on email chains and memory. That is one useful takeaway from this piece on regulatory compliance for medtech. The same operating principle applies here.
Practical rule: The day an underpaid NSA claim posts, the practice should decide three things: whether the claim is federally protected, whether the dollars justify escalation, and what evidence the payer is likely to attack.
What winning groups do differently
Practices with stronger IDR results usually share three habits:
- They pick disputes strategically. They do not send every underpayment into the same workflow. They focus on claims with clear federal protection, meaningful dollar variance, and facts that can be proven cleanly.
- They build the record early. Operative notes, call schedules, medical necessity support, coding logic, and payment comparison materials are gathered before deadlines create pressure.
- They argue the case the way a payer will defend against it. The submission addresses likely challenges up front instead of waiting for the other side to define the dispute.
Handled that way, IDR stops being a compliance headache and starts functioning as a controlled revenue recovery process.
IDR Eligibility What Claims Qualify and Which Get Rejected
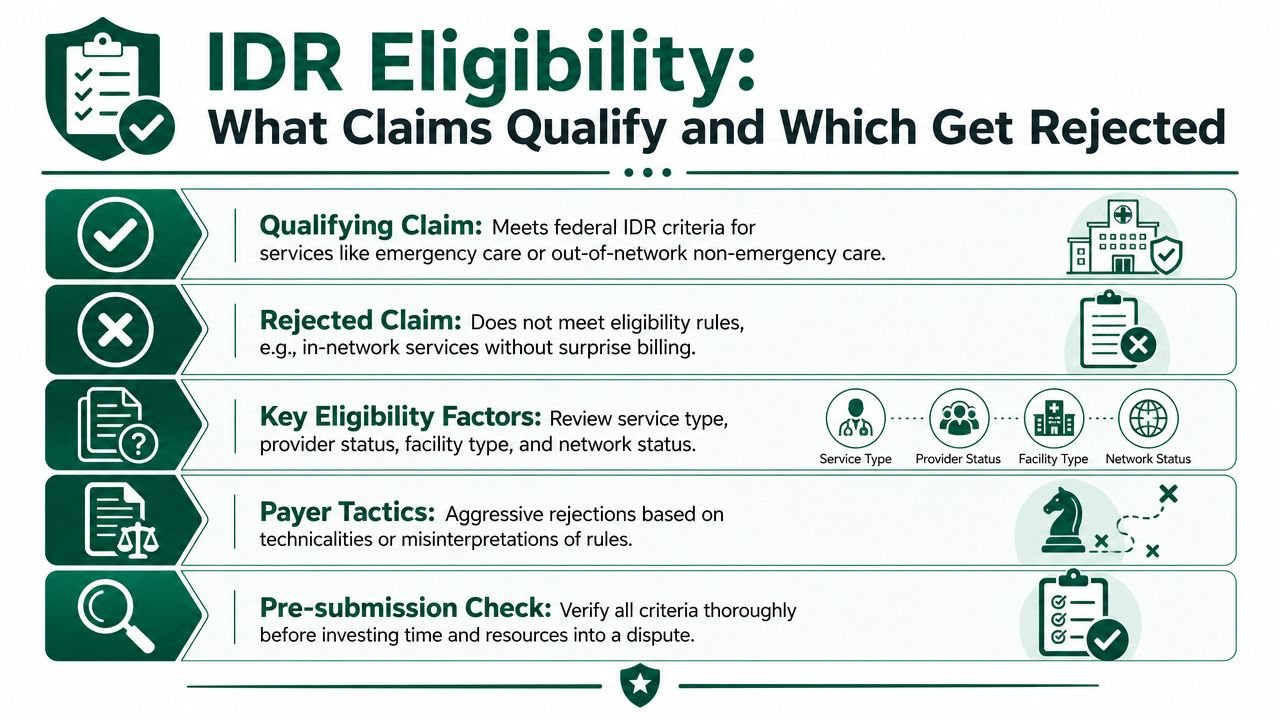
The biggest front-end mistake is assuming any out-of-network claim can go into federal IDR. It can't. If your team sends in disputes without strict screening, you'll spend staff time on claims that were never going to survive intake.
CMS says parties must attest that the item or service is within federal IDR scope. That matters because plans are actively attacking eligibility at the front end. A Georgetown 2025 early-data review found plans challenged 40% of cases as ineligible in the first half of 2025, and 22% of determinations were defaults because only one side submitted an offer and fee, according to CMS guidance on payment disputes between providers and health plans.
For a practice owner, that means this: the first financial decision isn't whether you can win. It's whether the claim belongs in the federal process at all.
Claims that generally belong in the conversation
At a high level, the federal framework applies to protected categories such as:
- Emergency services where the patient protections attach under the NSA
- Certain non-emergency services furnished by out-of-network clinicians at in-network facilities
- Air ambulance services that fall within the federal protection structure
If your physicians provide hospital-based care, on-call specialist services, or facility-based professional services, these are the categories your team needs to recognize quickly.
Claims that often get kicked out
Many disputes fail before substance is ever reviewed. Common reasons include:
- The claim isn't in federal scope
- The service setting doesn't fit the protected category
- The provider or facility status doesn't line up with the statute
- The filing package lacks the claim details or attestations CMS expects
- The wrong party submits, or one side fails to complete its required offer and fee steps
A surprising number of losses are procedural, not analytical.
If your staff can't explain in one sentence why the claim is eligible for federal IDR, they probably shouldn't file it yet.
A triage checklist we use in practice
Before anyone invests time in a dispute, make sure your team can answer these questions:
| Screening point | Why it matters financially |
|---|---|
| Is this a protected service category under the NSA? | If not, staff time goes into a dead claim |
| Was the physician out of network and the facility status relevant to federal scope? | This is where many payer eligibility attacks start |
| Do we have the payer's initial payment or denial and claim identifiers organized? | Missing detail slows filing and increases default risk |
| Is the payment variance large enough to justify pursuit? | Not every technically eligible claim deserves the same attention |
| Can we support the billed service level, modifiers, and medical record? | Weak coding support hurts leverage before arbitration even starts |
This is also where coding discipline matters to owners. If your physicians billed emergency E/M levels such as 99284 or 99285, or procedural services that depended on modifiers like -25, -59, or anesthesia modifiers such as AA, QK, QX, or QZ, your dispute strategy has to start with whether that coding is defensible. An eligible claim with weak coding still produces a weak case.
Practices that want a plain-language refresher on where patient protection rules intersect with reimbursement should also review this breakdown of balance billing requirements. It helps sharpen the line between a collectible payment dispute and a claim your team shouldn't push into federal IDR.
The Federal IDR Process Timeline and Fees
A payer posts an underpayment on Monday. By the time your billing lead, coding lead, and outside counsel all weigh in, the filing window is gone. The claim may still be defensible, but the revenue is effectively written off because the process failed before the merits were ever reviewed.
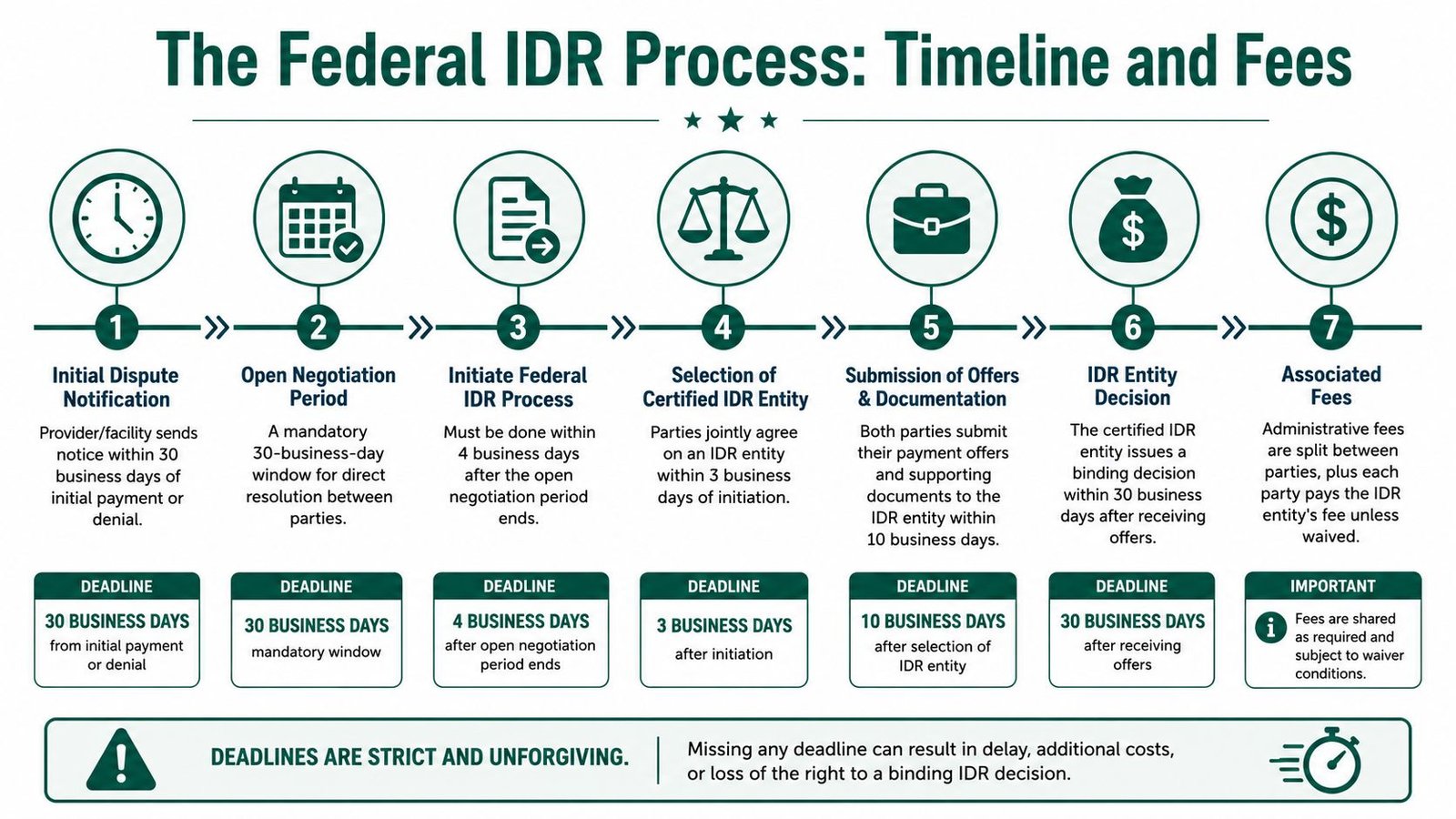
That is why strong IDR performance starts with clock management. Under the No Surprises Act, parties first go through a 30-business-day open negotiation period. If no agreement is reached, the party seeking federal IDR has only 4 business days to initiate the dispute. After the certified IDR entity issues its determination, payment must be made within 30 calendar days.
Those deadlines sound manageable on paper. In practice, they punish any physician group that treats IDR as a side task.
The operational risk is not evenly distributed across the timeline. The biggest losses happen at two points. First, teams fail to flag the underpayment fast enough to start open negotiation cleanly. Second, they wait until the negotiation period is ending to decide whether the claim is worth pursuing. At that stage, payer tactics matter. Carriers know that a short filing window favors the side with tighter internal controls, and they often benefit when provider documentation, coding review, and decision-making are scattered across departments.
A workable sequence looks like this:
- Initial payment or denial is posted and reviewed quickly.
- Open negotiation is sent with the right identifiers and dates.
- The practice decides during negotiation, not after it, whether the claim will go to IDR if the payer holds its position.
- The federal IDR filing is submitted before the 4-business-day window closes.
- The evidence package and formal submissions are completed on schedule.
- The certified IDR entity issues a determination.
- Any additional payer amount due is tracked through payment receipt and reconciliation.
This is a revenue cycle discipline issue, not just a legal one.
Fees still matter, but they usually are not the reason a good claim underperforms. Georgetown researchers estimated that by 2024, the IDR system had generated at least $5 billion in total costs since launch, including about $218 million in administrative fees, an additional $10 million for air ambulance disputes, and roughly $2.24 billion in extra payments for services during 2023–2024 alone. The same Georgetown analysis reported $885 million in fees collected to finance dispute resolution, and that CMS later reduced the administrative fee from $115 per party per dispute to $15 per party per dispute, according to Georgetown's review of the substantial costs of NSA arbitration. Georgetown also notes that CMS said in May 2026 that final rules were intended to clarify timelines and improve communication in the federal IDR process.
For practice owners, the financial question is straightforward. The filing fee is visible, but internal waste costs more. A claim that sits unworked for two weeks, gets escalated twice, and misses a deadline has already consumed staff time without any recovery. A claim that is identified early, triaged correctly, and filed with a clear owner has a much better margin profile, even if the disputed amount is modest.
We usually see four cost drivers behind weak IDR performance:
- Late identification of underpaid eligible claims
- Inconsistent or poorly documented open negotiation notices
- Evidence gathering that starts after the filing clock is already running
- No single owner for initiation, submission, and post-award follow-up
A simple control sheet fixes more of this than many practices expect. Track the initial payment or denial date, the date open negotiation was sent, the negotiation end date, the last day to initiate IDR, the assigned owner, the evidence packet status, and the post-decision payment follow-up date. Keep that tracker inside the same workflow your team already uses for denials and underpayments, not in a separate spreadsheet no one checks.
If your process still lives in email threads, it is too easy for a winnable dispute to expire. A tighter operating model for No Surprises Act compliance workflows helps reduce that risk and turns IDR from an occasional scramble into a repeatable revenue recovery function.
Preparing a Winning IDR Submission Package
Winning isn't random. The provider side performs best when the submission is built like a case, not a complaint.
The most important strategic fact is this: a Commonwealth Fund report on the first half of 2023 found that providers, facilities, or air ambulance providers won about 77% of resolved cases. When providers won, the median award was 322% of the QPA. When payers won, the median was 100% of the QPA, according to the Commonwealth Fund's report on how the dispute process has favored providers in resolved cases.
That doesn't mean every provider should file every dispute. It means a well-prepared case can materially outperform the payer's starting number.
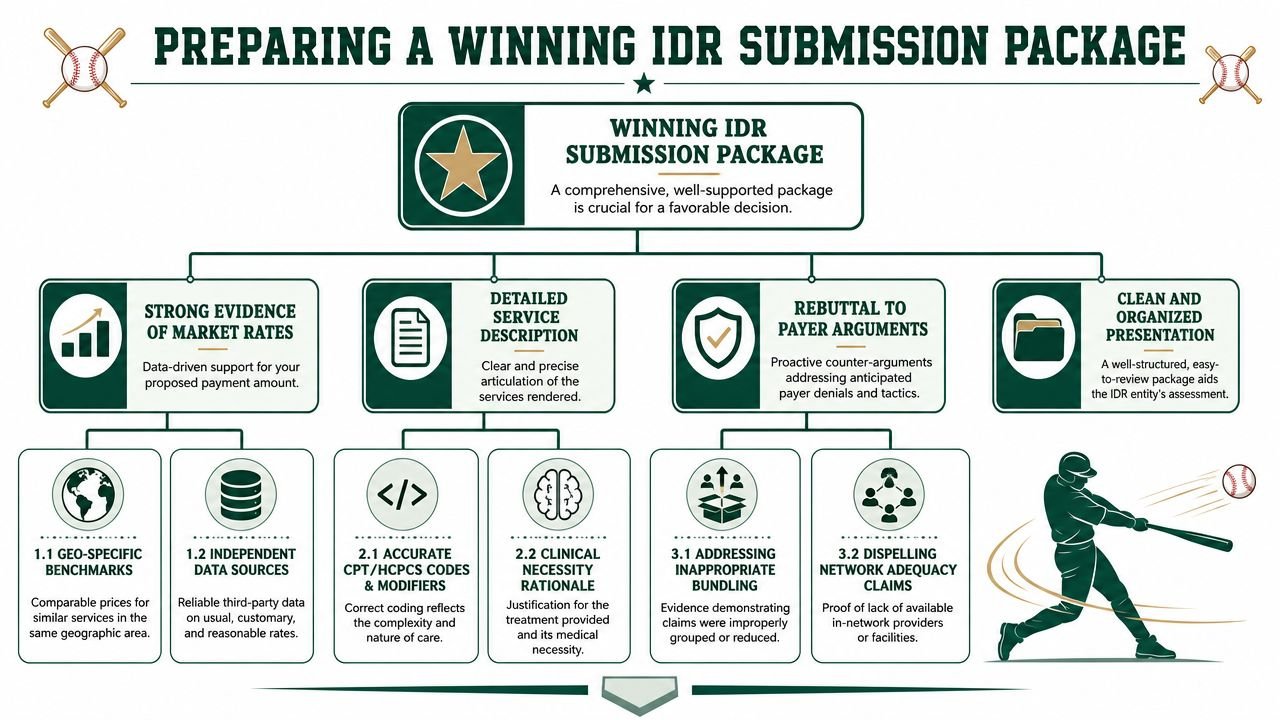
What a strong package includes
A winning submission usually has four traits.
It explains the service, not just the charge
Payers often reduce a claim to a line item. Your package has to restore clinical and operational context.
For example, if the dispute involves a higher-acuity emergency physician service such as 99285, don't just list the CPT code. Show the medical record facts that support the intensity of history, exam, decision-making, and resource use. If the dispute involves anesthesia, support any relevant modifiers such as AA, QK, QX, or QZ with staffing and concurrency records. If it's a procedure with modifier -22, -59, or -25, show why that modifier changed the payment logic.
Owners should care because unsupported coding shrinks negotiating advantage long before the IDR entity reviews the dispute.
It addresses the QPA without treating it as untouchable
The payer will often lean heavily on the Qualifying Payment Amount. You don't win by ignoring it. You win by contextualizing it.
Your team should be ready to show why the payer's number doesn't fully reflect the service at issue, based on the circumstances of the care, physician skill, service complexity, or setting. A bare statement that your charge is higher isn't persuasive. A structured explanation tied to the facts of the encounter is.
The best provider submissions don't sound offended. They sound organized.
It makes complexity visible
Many disputes are lost because the package assumes the reviewer will infer difficulty from the code itself. They won't.
Spell out details such as:
- Patient acuity and why the encounter demanded more physician effort
- Clinical complexity of the procedure or episode
- Facility context, including why the setting matters
- Physician training and experience when relevant to the service delivered
- Records that support modifiers and distinct procedural work
For specialty groups, that can mean very different evidence. A cardiology claim may need procedural and emergent context. An orthopedic dispute may need clear operative detail and global-period awareness. A pain practice may need to defend distinct services and modifier usage. A spinal case involving a code such as 22853 needs much more than a screenshot of the remittance.
How to organize the file so the reviewer can use it
The cleanest packages usually follow a simple order:
- Cover summary with the provider's offer and a short rationale
- Claim detail sheet with dates, codes, modifiers, and payment history
- Clinical support from the record
- Coding support for the billed CPT and modifiers
- Rebuttal points addressing the payer's likely arguments
Here's a useful internal test. If an IDR reviewer spent only a few minutes on your packet, would they know why your number is the better choice? If the answer is no, the package isn't ready.
Practices that already struggle with weak reconsiderations and payer responses usually have the same problem in IDR. The appeal file lacks a clear thesis. This resource on how to appeal a denied insurance claim effectively is a good model because strong appeal thinking translates directly into stronger arbitration submissions.
Common Payer Strategies and IDR Pitfalls to Avoid
Most payers don't need to beat you on substance if they can beat you on friction. That's what makes recurring IDR pitfalls so costly. They delay payment, increase staff burden, and push practices into accepting weak settlements just to clear the queue.

One common pattern starts with classification. The payer argues the claim isn't in scope, not because the facts are strong, but because it knows eligibility fights consume time. Another starts with documentation volume. The plan asks for detail your team should have assembled earlier, then benefits when the internal scramble causes a missed deadline or a weak filing.
The tactics we see most often
Low-information QPA positioning
The plan cites its payment benchmark as if the number ends the conversation. If your package doesn't directly respond, the payer's figure becomes the default frame for the dispute.
Bundling logic that weakens the claim
We've seen disputes get muddied when payers characterize separate services as if they were naturally grouped. That doesn't always happen through a formal denial code. Sometimes it happens through the narrative they build around what they believe should have been paid together or reduced.
If your physicians regularly bill combinations involving modifiers like -59 or -25, clean documentation converts into revenue.
Delay pressure
Not every delay is accidental. Some disputes drag because the payer benefits when your team is overloaded, uncertain about ownership, or inconsistent about portal follow-up. The goal isn't always to win on the merits. Sometimes it's to make pursuit feel not worth it.
Keep every notice, portal message, payment record, and submission copy in one dispute file. If the record is fragmented, the payer already has an advantage.
Pitfalls inside the practice
Some of the worst losses are self-inflicted:
- The coding team and follow-up team work from different facts
- The physician record doesn't support the billed intensity
- Nobody owns post-negotiation escalation
- The practice files too many low-value disputes and starves the important ones
- Staff assume prior appeal language is good enough for IDR
The fix isn't heroic effort. It's repeatable discipline. Build a standard evidence set by specialty, preserve records early, and use templates that force the team to answer the payer's likely objections before the dispute is filed.
Integrating IDR Into Your Revenue Cycle Management
IDR works best when it's part of your core revenue cycle, not a side project. That's especially true now that a May 2026 CMS final rule allowed providers to batch up to 50 items and services into a single dispute, a change reported by the American Hospital Association in its summary of the final rule updates to the IDR process.
That batching rule matters for owners because it changes staffing math. High-volume specialties can reduce per-dispute administrative friction if claims are identified, grouped, and documented correctly. But batching only helps practices that already know how to spot qualifying claims and maintain clean claim-level support.
The business question owners should ask
You don't need to ask whether IDR exists. You need to ask whether your current RCM setup can execute it without harming other parts of the business.
A workable internal IDR program needs:
- Fast underpayment identification
- Deadline control
- Coding and clinical documentation alignment
- Payer follow-up after determination
- Leadership reporting on recoveries, write-offs, and aged dispute inventory
If your team struggles with denials, appeal consistency, or aging control now, IDR usually exposes those weaknesses faster. This is why an integrated approach to revenue cycle management operations matters. The same systems that improve clean claims and denial prevention also improve your odds in high-stakes disputes.
For many independent groups, the build-versus-buy question isn't philosophical. It's financial. If internal staff can manage IDR accurately and on time, keep it in-house. If not, every missed window and weak submission becomes another preventable loss.
Frequently Asked Questions About the IDR Process
Is the IDR process worth it for a smaller independent practice
It can be, especially if your practice handles high-value hospital-based or procedural claims. The key isn't size. It's claim value, eligibility discipline, and whether your team can move quickly enough to protect the filing window. For some groups, a small number of well-chosen disputes justifies the effort. Practices in specialties like orthopedics often feel this more acutely because a handful of underpaid cases can distort monthly collections.
What's the real cost of pursuing IDR
The bigger cost is staff time and execution quality, not just filing fees. If your team can identify the right claims, preserve evidence early, and submit clean packages, the economics are usually better. If the process is handled inconsistently, the hidden cost shows up in A/R drag, rework, and weak settlements.
What happens if we lose
If the payer's offer is selected, you receive that amount. In many situations, that's close to where the claim would have landed anyway if you had accepted the underpayment without escalation. A major risk is wasting internal effort on claims that weren't screened or documented properly.
Should our physicians be involved in every dispute
Not every time, but physician input is often decisive for higher-acuity or more complex cases. The best use of physician time is targeted. Have doctors validate the clinical facts that explain complexity, setting, necessity, and any modifier-sensitive work. Administrative staff can organize the file, but physician documentation often gives the submission its force.
If you're unsure whether your current billing team is protecting revenue on No Surprises Act claims, get an outside read before another filing window slips by. Happy Billing works with independent practices that need tighter denial control, faster cash flow, and better recovery on difficult claims. If you want to see where your process is leaking money, request a free, no-obligation billing audit.