Medical Billing for Small Practice: A Physician’s Guide
Medical billing for a small practice is a revenue function, not an administrative task. Approximately 80% of U.S. medical bills contain some kind of error, and practices commonly lose 4% to 5% of revenue to leakage from routine mistakes, which is why billing problems show up first in cash flow, denials, and A/R pressure.
If your schedule is full but deposits still feel inconsistent, the issue usually isn't demand. It's the handoff between front desk, clinical documentation, coding, claims, denials, and collections. A small practice can stay busy all month and still starve financially when claims go out with bad eligibility data, incomplete documentation, missing modifiers, or weak follow-up.
Owners often notice the symptom before the cause. Payroll feels tighter than it should. Old claims linger. Patient balances rise. Staff say they're “caught up,” yet your aging report says otherwise. That's why medical billing for small practice operations has to be managed like an operating system for cash, not a clerical afterthought.
The useful question isn't “Do we have someone submitting claims?” The useful question is whether your process is producing acceptable A/R days, denial rates, and first-pass performance. If it isn't, you either fix the workflow or hand it to a team that can.
Why Your Practice's Financial Health Depends on Billing
A common small-practice scenario looks like this. Patient volume is steady. Providers are productive. The practice should be healthy. Yet the bank balance says otherwise, and nobody can explain why reimbursement feels slower than the work being done.
That disconnect usually traces back to billing discipline. According to an Aptarro medical billing industry summary, approximately 80% of U.S. medical bills contain some kind of error, and U.S. practices commonly lose 4% to 5% of revenue to leakage from those routine mistakes. For an independent practice, that isn't abstract waste. It's delayed payroll flexibility, slower hiring, tighter vendor payments, and more owner time spent reviewing reports instead of growing the business.
Billing is the cash engine
Medical billing for small practice owners should be viewed the same way you view provider scheduling or payer contracting. If it fails, revenue stalls.
A bad claim doesn't just create one problem. It creates a chain reaction:
- Front-end mistakes create denials: Wrong subscriber data or inactive coverage turns a clean visit into rework.
- Coding defects slow cash: Missing documentation support, incorrect CPT selection, or modifier misuse pushes claims out of the paid queue.
- Weak follow-up inflates A/R: Claims that aren't worked quickly age into harder collections.
- Poor patient collections shift burden downstream: If copays and balances aren't addressed early, the practice carries avoidable receivables.
Practical rule: If your team treats billing as “posting charges and waiting,” your practice is operating reactively, not financially.
Owners don't need to code every chart. They do need to know where revenue is being lost and what operational choices cause it. That's the difference between a practice that looks busy and a practice that converts work into cash.
What owners should monitor
The first discipline is visibility. You need to connect clinical production to financial output, then compare what should have been collectible to what hit the bank.
A strong starting point is reviewing your broader RCM strategy for physician practices. That lens matters because billing performance isn't isolated to the back office. It starts at scheduling and check-in, then shows up later in denial patterns and A/R aging.
The owners who stay ahead of reimbursement problems don't wait for month-end surprises. They ask harder questions earlier. Why are denials rising? Which payer is slowing? Are front-end edits catching preventable errors? Is a coding issue isolated to one provider, one CPT family, or one location?
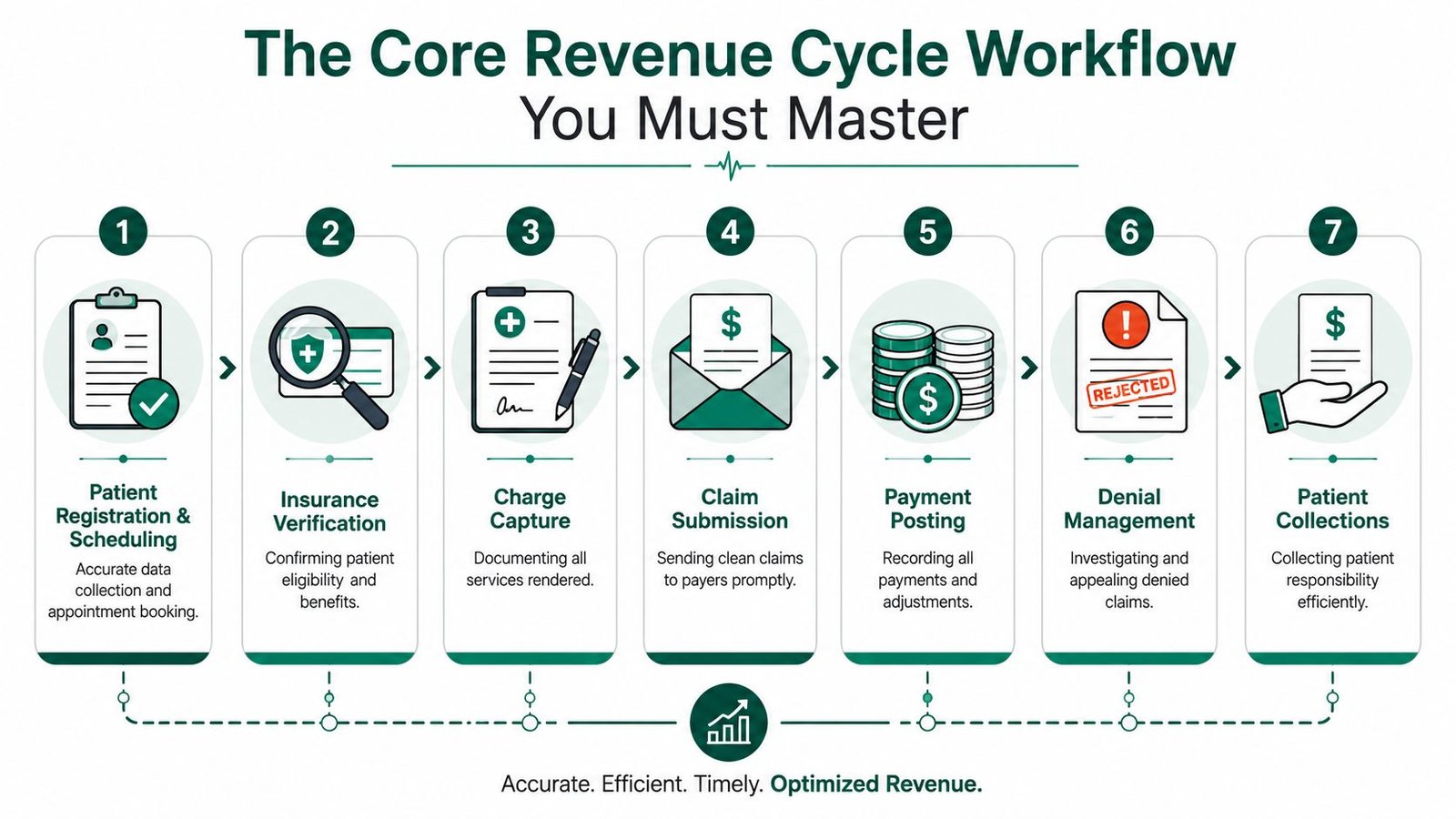
The Core Revenue Cycle Workflow You Must Master
The cleanest revenue cycles are boring. Registration is accurate, eligibility is checked before the visit, documentation supports the charge, claims go out fast, denials are worked quickly, and patient balances don't sit untouched.
That isn't luck. It's workflow control.
The front end decides whether cash moves fast
The most impactful control in a small practice is a standardized front-end workflow that combines real-time insurance eligibility checks with clean-claim scrubbing. Industry guidance for independent practices notes that this reduces insurance-data errors and catches coding defects before submission, improving first-pass acceptance and shortening A/R days, as outlined in this small-practice billing workflow guide.
If I'm diagnosing a struggling office, I start here before I look at anything else. A front desk that verifies eligibility in real time, confirms coverage details, and collects patient responsibility up front prevents a large share of downstream cleanup. A front desk that “checks later” creates a denial factory.
Three owner-level controls matter most:
Registration discipline
Demographics, subscriber data, and plan details have to be right before the encounter is closed. If they aren't, your billing team spends time repairing avoidable defects instead of accelerating cash.Daily claim movement
Claims should leave the practice promptly. A charge that sits unbilled is silent A/R growth.Weekly unpaid-claim review
Don't wait for monthly close. Review unpaid and denied claims weekly so patterns surface while they're still fixable.
Practices that shorten A/R usually don't win on heroic collections work. They win by preventing defects before the claim ever leaves the system.
The back end is where discipline shows up
Payment posting, denial management, and patient collections tell you whether your process is controlled or improvised. If posting lags, you lose visibility. If denials aren't categorized well, you can't tell whether the problem is eligibility, coding, authorization, or payer behavior. If patient balances aren't worked consistently, self-pay A/R becomes a second unmanaged business inside the practice.
A practical operational map looks like this:
| Workflow stage | What the owner should ask |
|---|---|
| Scheduling and registration | Are staff capturing complete insurance and demographic data every time? |
| Eligibility and benefits | Is coverage verified before the visit, not after the denial? |
| Charge capture | Does documentation support the CPTs billed? |
| Claim submission | Are scrubbers catching obvious defects before claims go out? |
| Payment posting | Are payments and adjustments posted quickly enough to expose underpayments? |
| Denial follow-up | Are denials worked by root cause, not one-off reactions? |
| Patient collections | Are copays and balances addressed early and consistently? |
If your internal team is overloaded, even simple tooling can help tighten the receivables side. For example, teams looking to automate A/R with Retriever may find useful ideas around structured follow-up and receivables workflow design.
For a deeper look at tightening handoffs across the cycle, review these revenue cycle workflow improvements.
Decoding Common Revenue Leaks and Denial Traps
Most small practices don't lose money because of one catastrophic billing failure. They lose it through repeated, familiar mistakes that nobody fully owns. The same denial reason appears every week. The same payer keeps rejecting the same service family. The team appeals some claims, writes off others, and never fixes the process that caused them.
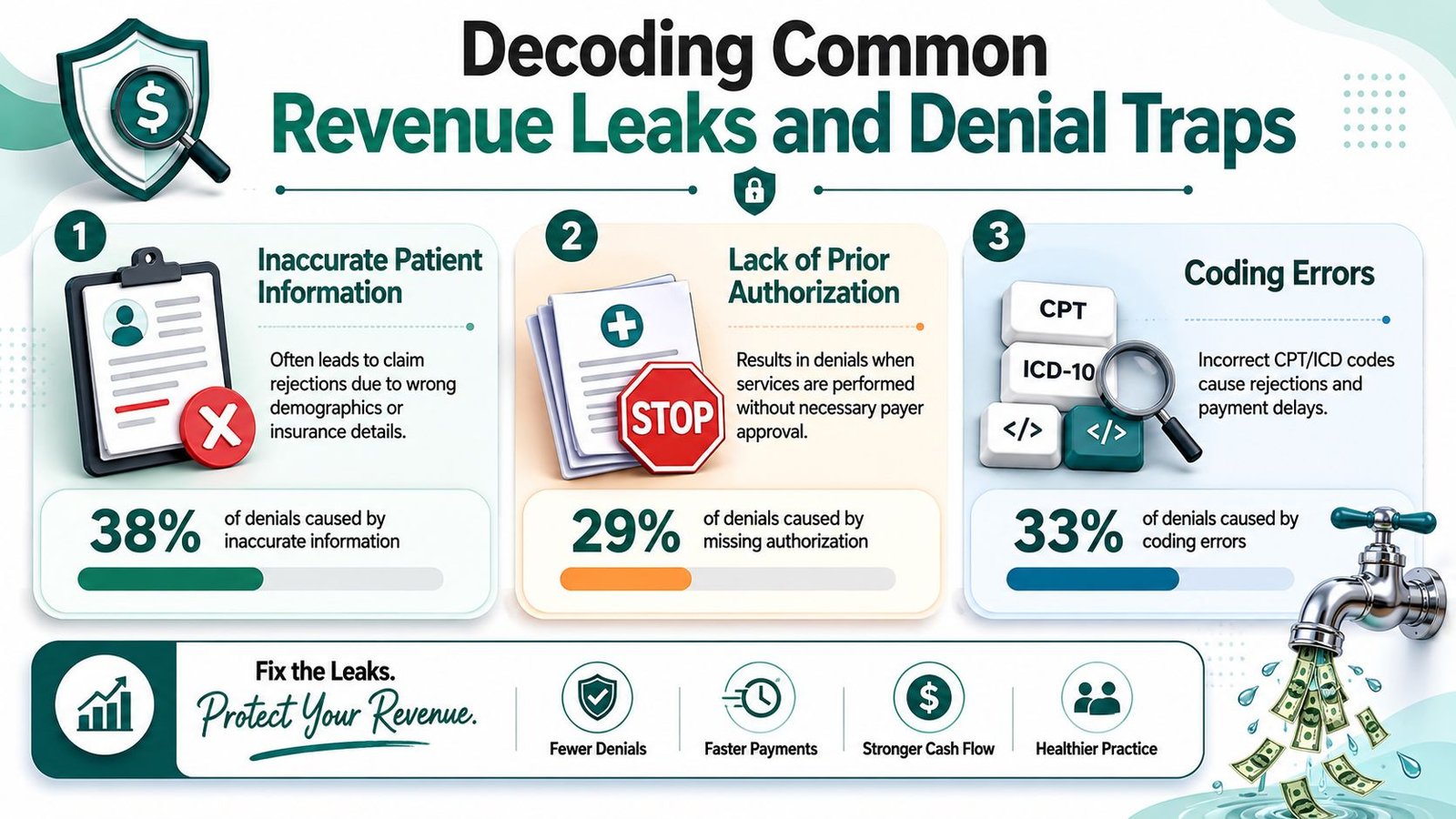
Coding errors that look small but pay badly
A classic example is the misuse of modifier 25 on an E/M service billed with a minor procedure. Under CMS and many payer policies, modifier 25 supports payment only when the E/M service is significant and separately identifiable from the procedure. If your documentation doesn't support that distinction, the payer may deny the E/M or recoup it later.
The owner-level issue isn't the modifier itself. It's what repeated misuse tells you. It usually means one of three things:
- Provider documentation isn't aligned with coding expectations
- Internal review rules are too weak before claim release
- The practice is relying on habit instead of payer-specific discipline
The same logic applies to procedural billing where modifier 59, modifier 24, modifier 57, or global-period edits come into play. If these are handled inconsistently, you don't just get denials. You create audit risk and underpayment risk.
Authorization gaps are expensive because they are avoidable
Authorization failures are one of the most frustrating forms of revenue leakage because many of them start before the patient is even seen. Imaging, behavioral health, anesthesia-adjacent services, and procedural specialties all face this in different ways. A missing authorization number, a mismatch between the authorized service and the billed service, or a date-of-service discrepancy can turn a valid clinical service into a nonpayable claim.
This is why generic “submit clean claims faster” advice often falls short. A claim can be perfectly formatted and still be uncollectible if the payer expected authorization, supporting records, or specialty-specific documentation.
A denial is only a back-end event on paper. In practice, many denials were created days earlier at scheduling, intake, or charge review.
Denial management fails when it stays reactive
Many practices treat denials as a queue to clear rather than a pattern to fix. That approach keeps staff busy without improving the system.
Better denial management means sorting by root cause and financial impact. Not every denial deserves the same response. Some should trigger immediate correction and staff retraining. Some should trigger payer escalation. Some should trigger an outsourcing decision because the volume or specialty nuance is beyond what a small in-house team can handle efficiently.
A short diagnostic table helps:
| Denial area | What it usually signals |
|---|---|
| Eligibility | Front-desk verification failure |
| Authorization | Scheduling or referral workflow gap |
| Coding and modifiers | Documentation or coding review weakness |
| Timely filing | Staffing, workflow delay, or claim hold issue |
| Medical necessity edits | Payer policy mismatch or incomplete records |
If you're seeing recurring patterns, your first move shouldn't be more manual work. It should be process redesign. This medical billing denial management resource is a useful reference point for evaluating whether your current denial workflow is preventing repeat losses.
The In-House vs Outsourcing Decision Framework
The right question isn't whether outsourcing is better in theory. The right question is whether your current setup is producing acceptable financial outcomes with acceptable management burden.
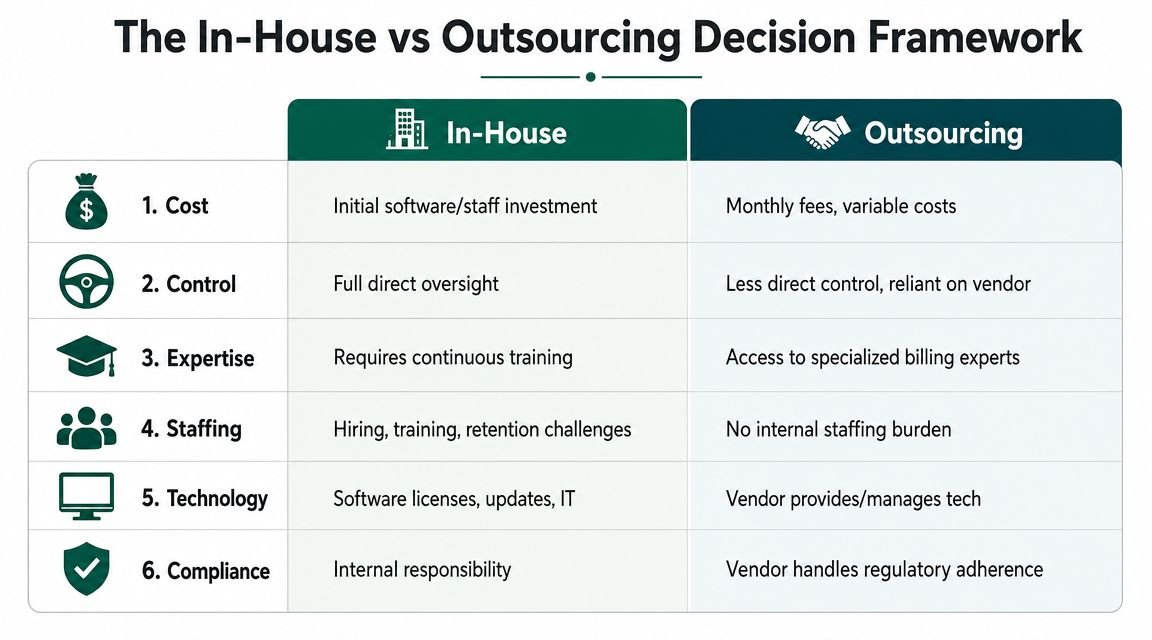
A practice should usually keep billing in-house when leadership has strong visibility, the workflow is stable, and the team can manage payer complexity without constant rework. A practice should look seriously at outsourcing when ownership is spending too much time fixing billing issues, key metrics are moving the wrong way, or specialty-specific denials keep recurring despite software and staffing.
When in-house still makes sense
Modern billing platforms have made in-house operations more feasible. The shift from manual work toward integrated digital tools such as athenaOne has helped practices automate claim creation, tracking, and workflow management, as discussed in this overview of medical billing software for small practices. But automation doesn't solve denial complexity by itself.
In-house can work well when:
- Your team knows your specialty well: Orthopedics, mental health, cardiology, and anesthesia all generate distinct payer friction.
- Leadership gets usable reports: If you can see claim status, denial categories, and A/R movement clearly, you can manage.
- Turnover is low: Revenue cycle performance falls quickly when billing knowledge lives in one employee's head.
When outsourcing is the cleaner decision
Outsourcing becomes more attractive when the practice needs expertise and consistency more than direct day-to-day control. That tends to happen in independent groups where physicians are already carrying clinical, staffing, and payer burdens.
Good trigger questions include:
- Are A/R days moving up without a clear explanation?
- Are denials repeating by payer, CPT family, or provider?
- Is your biller spending more time fixing errors than preventing them?
- Does one employee hold too much billing knowledge?
- Are prior authorization and modifier issues specialty-specific enough that general billing support isn't enough?
If your billing operation depends on one experienced staff member never being absent, you don't have a system. You have a key-person risk.
The trade-off is straightforward. In-house gives you tighter daily control. Outsourcing can give you deeper expertise, better redundancy, and less staffing drag. Neither model is automatically superior. The better model is the one that improves your revenue metrics without creating management chaos.
Technology also matters here because outsourcing decisions often overlap with broader operations and vendor dependence. If you're weighing what functions belong internally versus externally, ARPHost's IT outsourcing guide offers a practical way to think about support burden, specialization, and operational risk.
For a side-by-side look at what practice owners should compare, this guide to in-house vs outsourced medical billing is worth reviewing. If you want a real answer, compare your current A/R days, denial patterns, first-pass performance, and staff time spent on rework. That tells you far more than vendor promises.
Choosing Your Billing Technology and Ensuring Compliance
Software shouldn't be purchased because it looks modern. It should be chosen because it fits your workflow, reduces defects, and gives management real visibility into claims, denials, and collections.

Buy for workflow fit, not feature count
Small-practice guidance consistently points to the same evaluation criteria: integrated EHR and billing, real-time claim-status tracking, code scrubbing, payment posting automation, analytics, and patient payment tools. The core point is that software should be judged by whether it lowers A/R days and improves first-pass acceptance, not whether it merely digitizes the same broken process, as explained in this AdvancedMD review of reimbursement challenges for small practices.
When I review software decisions, I look for a few essential requirements:
- Integrated clinical and billing workflow: Duplicate entry creates mismatches between documentation and claims.
- Real-time claim visibility: Owners need to know where claims are stuck and why.
- Denial analytics: If the system can't show denial patterns clearly, you can't manage root causes.
- Patient payment tools: Estimates, statements, and portals matter because patient balances are now a meaningful part of cash flow.
A practice management platform also has to fit the actual operating environment of the office. Teams comparing hosted and cloud-based options may find Cloudvara's practice management solutions useful for thinking through access, maintenance burden, and operational flexibility.
Compliance is part of revenue protection
HIPAA, user permissions, audit trails, and secure handling of PHI aren't separate from billing performance. They are part of it. Weak access control and poor documentation discipline create operational noise, increase correction work, and expose the practice to preventable risk.
From an owner's perspective, compliance questions should be practical:
| Compliance area | What to verify |
|---|---|
| User access | Can staff only see what they need for their role? |
| Audit trail | Can you track who changed claims, balances, or demographics? |
| Data handling | Is PHI protected in transmission, storage, and daily workflow? |
| Documentation linkage | Can the claim be tied back clearly to the supporting chart? |
CMS expectations, payer edits, and AAPC coding standards all point in the same direction. Consistent documentation, appropriate code selection, and traceable workflows protect revenue. They also make appeals stronger when payment is challenged.
If you want a broader framework for evaluating automation without losing control, review these revenue cycle management automation considerations.
Specialty-Specific Billing Nuances That Impact Your Bottom Line
Generic billing advice breaks down fast once specialty rules take over. That's where many independent groups lose money. The claim isn't denied because your team failed to submit it. It's denied because the specialty-specific rule was missed upstream.
Practice-level payer friction increasingly comes from service-line-specific rules. In mental health, prior authorization is a major denial source, while procedural specialties such as orthopedics deal with modifier complexity and global-period edits, as discussed in this specialty-focused medical billing software guidance.
Mental health and behavioral health
Behavioral health groups often think their challenge is standard claim submission. In reality, the harder problem is authorization capture and documentation alignment. Session limits, payer-specific utilization management, and medical necessity support can determine whether a clean claim gets paid at all.
CPTs such as 90791, 90834, 90837, and 90853 may look routine, but reimbursement risk often sits around authorization status, frequency limits, and documentation support. If the practice waits until denial posting to discover that an authorization lapsed, the billing team is already working from behind.
Orthopedics and procedural care
Orthopedic and pain practices live in a different denial environment. Global periods, procedure bundling, laterality, and modifier use matter constantly. A post-op visit billed separately during a global period, or a procedure submitted without the right modifier support, can produce denials that a generalist billing workflow won't catch consistently.
Codes vary by procedure family, but the operational risk is stable. The practice needs someone who understands when modifier 24, modifier 25, modifier 57, modifier 59, or anatomical modifiers change payment outcomes and when they don't.
Anesthesia and cardiology
Anesthesia revenue depends heavily on unit logic, time capture, concurrency, and modifier discipline. A technically submitted claim can still be financially wrong if base units, time units, or anesthesia modifiers don't align. Cardiology brings a different pattern. Diagnostic testing, interventional procedures, and imaging-related rules often require tighter charge review and better matching between documentation and claim construction.
Specialty billing isn't harder because it uses more codes. It's harder because one missed specialty rule can turn a clinically appropriate service into an avoidable denial.
If your practice sits in one of these high-friction specialties, a generic billing partner or generic internal workflow usually won't be enough. The right place to start is a specialty-specific evaluation of where your denials originate. You can review the relevant specialty billing areas here.
KPIs and FAQs for Practice Owners
If you only review total collections, you're managing too late. Owners need a small set of KPIs that show whether medical billing for small practice operations is healthy before cash problems become obvious.
The KPI dashboard that matters
Track these consistently:
Days in A/R
This tells you how quickly work turns into cash. If days rise, ask whether the cause is front-end defects, slower claim release, denial backlog, or weak follow-up.Denial rate
Review denials by payer, specialty area, provider, and root cause. A single blended percentage is less useful than pattern visibility.First-pass acceptance
This is one of the clearest indicators of billing quality. When it slips, rework rises and cash slows.Net collection performance
Owners should compare expected collectible reimbursement to what was collected after contractual adjustments and write-offs.
A KPI is only useful if someone owns the response. If denial rate rises, who investigates? If A/R days worsen, who changes workflow? If claims are edited repeatedly before submission, who is fixing the root cause?
Questions owners actually ask
Should I fix my in-house billing team first or outsource immediately
Fix in-house first when the issue is clearly operational and leadership can enforce change quickly. Outsource when problems are recurring, specialty-specific, or dependent on one or two people whose bandwidth is already maxed out.
What should I ask for in a billing performance review
Ask for claim lag, denial categories, A/R aging by payer, unpaid claims by reason, modifier-related denials, authorization-related denials, and where rework is entering the process. If a reviewer can't show root causes, you're getting commentary, not diagnosis.
How long does it take to know whether a billing change is working
You should see movement first in process indicators, then in financial outcomes. Cleaner front-end workflow, faster claim release, and better denial categorization usually appear before A/R improves meaningfully.
How do I know whether my specialty needs specialized billing support
Look at your denial mix. If problems repeatedly involve authorization rules, modifier use, global periods, anesthesia units, imaging edits, or payer-specific documentation standards, your practice probably needs specialty-aware billing, not general claim submission.
Happy Billing helps independent practices diagnose whether their billing operation needs repair or replacement. If you want a practical review of your denial patterns, A/R pressure, and specialty-specific revenue leaks, request a free billing audit or learn more about Happy Billing.