Choosing a Pain Management Billing Company: 2026 Guide
If you're choosing a pain management billing company in 2026, use a hard checklist, not a polished demo. The vendors worth taking seriously should be able to show first-pass clean claim performance above 98%, denial rates below 5%, and faster cash movement, because specialized pain management RCM has already proven those outcomes are achievable.
You're probably in the exact spot we see all the time. You've decided to outsource, you have two to four vendors on your shortlist, and every one of them says they “specialize” in pain management. That word means nothing until the company shows you how it handles your denials, your authorizations, your procedure mix, and your A/R.
This decision is financial, not administrative. A weak billing partner leaves money trapped in denials, stalls high-value procedures in pre-auth, and creates silent leakage around modifier use, charge capture, and appeals. A strong partner improves collections and cash flow speed. If you want a baseline on why outsourcing can work at all, these outsourcing billing benefits are a useful starting point. The rest of this guide is about something more important: how to separate a real pain management billing company from a generic RCM shop wearing specialty branding.
Moving Beyond Sales Pitches to a Real Evaluation
The fastest way to make a bad decision is to compare vendors by personality. The best presenter often loses once real claims hit payer edits.
We've seen physician owners focus on dashboard screenshots, friendliness, or a slightly lower fee, then spend months cleaning up the consequences. Pain management billing is unforgiving. You're dealing with procedural coding, strict documentation standards, payer-specific rules, prior authorization friction, and high-value claims that can't afford sloppy follow-up.
The benchmark that matters
A real pain management billing company should be judged against the level that specialized firms already reach. According to this industry review of top pain management billing companies, specialized partners report first-pass clean claim rates exceeding 98%, have reduced denial rates to below 5% within months of engagement, and some providers report A/R reduction within 24 days, with practices typically seeing revenue increases of 10-20%.
Those aren't vanity metrics. They tell you whether the vendor knows how to submit clean claims, prevent avoidable denials, and move money into the practice faster.
Practical rule: If a vendor can't tell you its current first-pass clean claim rate, denial rate, and A/R performance for pain management accounts, you're not evaluating a specialist. You're listening to a sales script.
Borrow a procurement mindset
Physician owners often evaluate billing partners too casually. You shouldn't. This is closer to selecting critical infrastructure than hiring a back-office service. The procurement logic in these CitySource Solutions MSP selection tips applies surprisingly well here: define your standards, ask for evidence, and inspect the operating model behind the promises.
Use that same discipline with billing vendors. Ask for sample reports. Ask how they escalate denials. Ask what happens when an epidural injection is denied for medical necessity. Ask who owns prior auth tracking and who is accountable when a missing authorization kills a claim.
What you are really buying
You are not buying claim submission. You are buying revenue protection.
That means a good partner should be able to show you:
- Specialty fluency with pain procedures and documentation risk
- Operational discipline around denials, appeals, and aging follow-up
- Visibility into what's happening by payer, provider, procedure, and aging bucket
- Accountability when performance slips
Everything else is secondary.
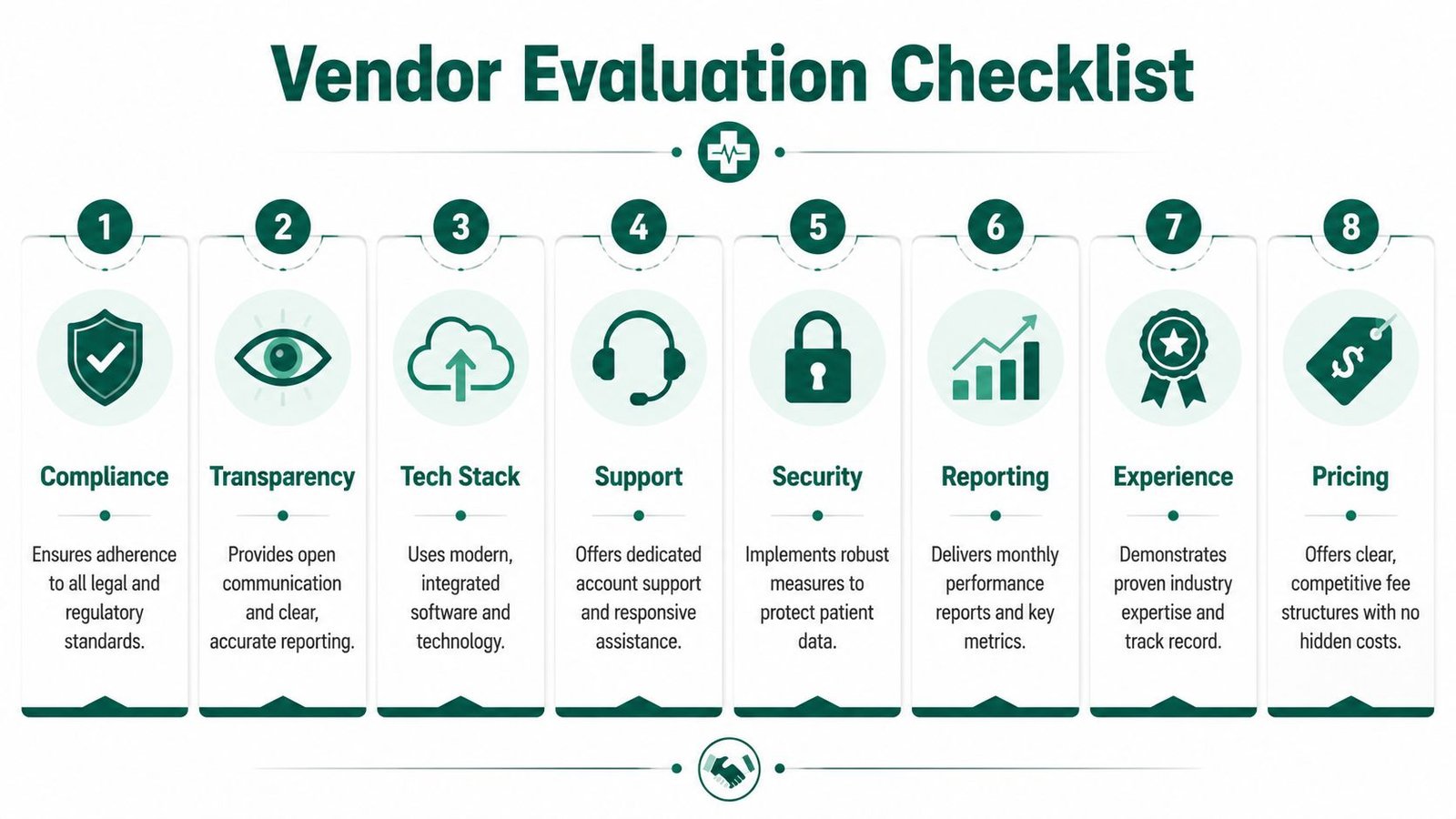
Your 8-Point Vendor Evaluation Checklist
The fastest way to compare a pain management billing company is to force every vendor through the same eight criteria. Don't let them control the conversation.
For context, this pain management CPT coding resource is worth reviewing before vendor interviews so you can pressure-test whether a company really understands your case mix.
Specialty procedure knowledge
Pain management is not generic professional billing. A vendor should be comfortable discussing common interventional coding scenarios like 62323 for epidural injections, 64493 for facet injections, and the modifier logic that affects payment.
What good looks like
- They can explain how they validate documentation before coding high-value procedures.
- They understand when modifier 59 may become a payment issue because the underlying documentation doesn't support distinct procedural service.
- They know that time-based services, injections, implants, and staged care plans create different denial patterns.
- They can discuss spinal cord stimulator trial billing, global-period exposure, and payer scrutiny without sounding like they're reading from a cheat sheet.
What to watch for
- They only talk about “accurate coding” in broad terms.
- They avoid specific CPT examples.
- They rely on your staff to explain specialty nuances.
- They can't explain how they handle anesthesia-related modifiers such as QK when your practice structure touches those workflows.
Denial management process
Weak vendors are easily exposed in this environment. In-house pain management billing often runs into 20-25% denial rates, and nearly 30% of denied claims are tied to coding and documentation mistakes. Expert partners use AI-powered scrubbing and real-time automation to reach 95%+ clean claim rates on first submission, according to this pain management billing guide.
Ask to see the actual workflow, not a promise.
| Criteria | What good looks like | What poor looks like |
|---|---|---|
| Root-cause review | Denials are categorized by payer, code family, provider, and reason | Everything is labeled “payer issue” |
| Appeal ownership | A named team handles appeal prep and filing | Appeals are reactive or pushed back to your staff |
| Prevention loop | Denial trends feed back into edits and documentation training | The same denial repeats month after month |
| Timeliness | Follow-up starts fast and aging is visible | Old denials sit untouched in work queues |
If a vendor can't produce a sample denial root-cause report, assume they don't run one.
Prior authorization control
For pain management, prior auth failure is often a direct hit to cash flow. Injections, implants, and other procedural services can be clinically appropriate and still go unpaid if the authorization trail is weak.
A serious vendor should tell you:
- Who tracks the auth from order to approval
- Where status lives inside the workflow
- How expired or incomplete auths are flagged
- How clinical documentation gets tied back to the claim
A weak vendor says pre-auth is “front desk responsibility” and leaves it there. That creates finger-pointing, not reimbursement.
EHR and PM integration
The best billing company works inside your current environment, not against it. You shouldn't have to rebuild your operation to fix your revenue cycle.
What good looks like
- They can work inside your existing EHR and practice management setup.
- Charge entry, coding review, claim edits, and payment posting move through a consistent workflow.
- They can explain how they avoid duplicate work and lost information between clinical notes and billing.
What to watch for
- They want manual spreadsheets for core processes.
- They depend on exports and re-uploads for routine work.
- They can't explain how they reconcile charges against completed encounters.
Reporting transparency
If you can't see performance by payer, provider, and denial reason, you're outsourcing blind.
Ask for a sample monthly report and inspect it for:
- First-pass acceptance trends
- A/R aging by bucket
- Denials by reason code
- Appeal outcomes
- Unbilled encounters
- Credits and refunds
- Patient balance trends
A vendor that sends a one-page summary with collections only is hiding the operational picture.
Fee structure clarity
Pricing tells you whether incentives are aligned. If the contract is vague, the relationship will be expensive.
Good vendors spell out:
- What's included in the percentage fee
- What triggers extra charges
- Whether credentialing, old A/R, patient statements, and appeals are separate
- How they handle out-of-scope work
Poor vendors bury add-ons in the agreement and make margin on confusion.
Contract terms and exit rights
The contract should provide you with an advantage if performance slips.
Look for:
- Short initial terms or practical out clauses
- Clear termination language
- Data access rights
- A documented transition process
If a pain management billing company traps you in a long auto-renewal with poor exit language, it already told you how confident it is in its service.
References from similar practices
General medical references are weak evidence. You need references from practices that look like yours.
Ask for references from groups with a similar profile:
- Interventional pain mix
- Multi-provider setup
- Medicare and commercial payer blend
- Procedure-heavy revenue model
If they can't produce that, move on.
The Three KPIs That Reveal True Performance
Most vendor comparisons break down because practice owners ask broad questions and get broad answers. You need three hard KPIs. Nothing cuts through a sales pitch faster.

If you want a fuller scorecard, this guide on medical billing KPIs to track is a solid companion.
First-pass acceptance rate
This is your clean-claim truth serum. It tells you how often claims get through on the first try instead of bouncing back for preventable reasons.
For pain management, this matters because one coding error, one missing modifier, or one documentation mismatch can delay payment on procedures that materially affect the month's cash collections. If a vendor won't provide a clean definition of first-pass acceptance and the exact figure for pain management accounts, assume the number isn't good.
Days in A/R
A/R days tell you how long your money sits outside the practice. That affects payroll, expansion plans, physician compensation, and your ability to tolerate payer nonsense.
According to this 2026 discussion of pain management billing trends, AI adoption in RCM has risen by 22% in 2026, while pain specialties still lag at 14% adoption. The more useful point for you is operational, not trendy: advanced agentic AI paired with 24/7 human oversight has been shown to reduce A/R by up to 40%. That hybrid model matters more than “AI-powered” branding.
A vendor using automation without human review can create faster mistakes, not faster cash.
If you want a broader perspective on where automation pays off, this healthcare automation and ROI guide is worth reading.
Denial rate
A denial rate should be measured consistently and reviewed by category. One flat number isn't enough.
You want to know:
- How many denials are preventable
- Which payers are driving them
- Which procedures get hit most often
- How many denials are overturned on appeal
A good vendor treats denial rate as an operating metric. A bad one treats it as bad luck.
What to ask in one sentence
Ask each vendor this exact question: “Show me your current first-pass acceptance rate, your current denial rate, and your current average A/R performance for pain management clients, and explain how you calculate each.”
If they answer with adjectives instead of numbers and methodology, stop there.
Red Flags to Walk Away From Immediately
Some issues aren't negotiable. They're disqualifiers.
If you want a broader checklist of warning signs, review these medical billing company red flags.
Long lock-in contracts
If a company wants a long-term agreement with aggressive auto-renewal before it has proven performance, that's a control tactic. We've seen practices lose months trying to exit a bad billing relationship while claims age and staff morale drops.
Good vendors rely on execution, not legal handcuffs.
Percentage fees with fuzzy add-ons
Percentage pricing isn't automatically bad. Hidden extras are. If the proposal leaves room for separate fees on patient statements, old A/R, credentialing, appeals, reporting, or software access, your effective rate can drift fast.
Ask for every billable item in writing. If the answer is slippery, walk.
No pain management proof
A company that can't show specialty references, sample reporting, and detailed process answers is telling you it doesn't really do this work at the level you need.
Owner test: If the vendor can't talk intelligently about 62323, 64493, modifier 59, authorization tracking, and procedure-driven denial patterns, it isn't a pain management billing company. It's a generalist.
Weak operational ownership
Be careful with phrases like:
- “Your staff will help us with denials.”
- “We escalate as needed.”
- “Our coders review when necessary.”
- “Pre-auth is mostly on the practice side.”
That language usually means fragmented accountability. Fragmented accountability leads to missed follow-up, recurring denials, and avoidable write-offs.
Finalizing Your Choice with a Sample RFP
You are one meeting away from making an expensive mistake.
A polished demo can hide weak follow-up, shallow specialty knowledge, and vague accountability. Put the sales process on paper before you sign anything. A short RFP forces each billing company to answer the same questions, in the same format, with enough detail for you to compare operations instead of personalities.
Before you send it, get clear on your baseline. If you do not know what your current team costs in labor, software, write-offs, and missed collections, you cannot judge an outsourced proposal accurately. This breakdown of what outsourced medical billing can cost will help you frame the comparison.
Questions that force real answers
Use questions like these:
- Describe your denial workflow for pain management claims. Name the role that classifies denials, the role that works appeals, and how recurring denial patterns get turned into front-end edits or provider feedback.
- Explain your prior authorization process for injections, implants, and other procedure-heavy services. State where status lives, who checks it before the visit, and who owns it before claim submission.
- List your experience with our top commercial payers and Medicare Administrative Contractor rules for pain management claims. Be specific about payer edits, modifier problems, and documentation failure points.
- Provide a sample monthly report that includes payer-level denial trends, A/R aging by bucket, unbilled encounters, and provider-level production.
- Explain how you code and review procedure documentation for services such as 62323 and 64493, including modifier review when needed.
- Describe your EHR workflow and whether your team works inside our current system or requires a separate process.
- Outline your contract terms, termination rights, data access, report access, and transition support if the relationship ends.
- Provide references from pain management practices similar to ours in size, payer mix, and procedure volume.
What a strong answer sounds like
A credible vendor gives you names, steps, timeframes, and examples. They can explain who touches a claim after denial, how often unresolved claims are reviewed, what gets escalated, and what reporting the owner will see each month.
Generic language is a bad sign. Phrases like "we customize our workflow" or "we partner closely with your staff" usually mean the process is undefined or the burden stays on your team.
We have seen physician owners save themselves a bad contract by scoring written answers side by side before taking a final call. Do that. Build a simple scorecard for specialty fit, operational ownership, reporting, transition plan, and contract clarity. If a vendor cannot win on paper, they will not win in production.
The smartest final step
Ask one question before you choose anyone: What do you see in our current data, and what would you change first?
That answer separates operators from presenters. A capable pain management billing company should be able to review your current performance, point to likely leakage, and explain where cash is getting delayed. If the response stays high level, they have not done enough work to earn your trust.
Use the RFP to narrow the field. Then require each finalist to react to your actual numbers, your payer mix, and your workflow. That is how you find the billing partner that can protect revenue after the contract is signed.
FAQs From Pain Management Practice Owners
How do I know if a pain management billing company is actually specialized?
Ask procedure-specific questions. If the vendor can't discuss common pain management services, modifiers, prior auth failure points, and payer edits without getting vague, it's not specialized enough. Real specialty depth shows up in the details, not in the website headline.
Should I choose the vendor with the lowest percentage fee?
Usually not. The cheapest fee often hides weak denial management, poor reporting, limited prior auth ownership, or extra charges outside the base agreement. A slightly higher fee can be the better financial choice if the company protects collections, cleans up aging, and gives you visibility into performance.
How disruptive is switching billing companies?
It depends on handoff quality, data access, and whether the new company can work inside your current systems. The risk is manageable if you define ownership upfront for open claims, old A/R, payer enrollment status, and reporting access. The core problem isn't switching. It's switching without a documented transition plan.
Should I audit my current billing company before signing a new one?
Yes. You need a baseline before you compare alternatives. Otherwise, every sales pitch sounds plausible. We've seen practices discover that the actual issue was preventable denial leakage, weak follow-up discipline, or poor authorization control, not just “billing is slow.”
If you're comparing pain management billing companies, the best low-commitment next step is to benchmark the one you already have. Happy Billing offers a confidential, no-pressure free audit that helps you evaluate denial patterns, A/R drag, and revenue leakage before you sign with anyone.