Orthopedic Billing Services: Maximize Revenue
TL;DR: Orthopedic billing services help practices protect revenue that is routinely lost to coding detail, payer edits, and weak denial follow-up. In orthopedics, a small documentation gap can change reimbursement fast. A missed laterality modifier, an unsupported assistant surgeon claim, or a post-op visit billed inside the global period can turn a payable case into rework, delay, or write-off.
Orthopedic revenue cycle work is won or lost at the code level. The difference between average billing support and true specialty support shows up in specific decisions: whether the diagnosis supports medical necessity, whether the op note justifies modifier 59 or XS, whether a payer will deny 29826 as bundled, or whether a return-to-OR scenario supports modifier 78 instead of 79.
That is why practices looking at orthopedic billing services for specialty-specific RCM support should test vendors on real claim scenarios, not sales language. Ask how they handle CPT 27447 inside the global package. Ask what documentation they require before billing bilateral or staged procedures. Ask which denial categories they appeal first, and how often they correct claims before submission rather than after rejection.
General billing teams can submit claims and post payments. Orthopedic billing teams that perform well prevent avoidable denials before they hit A/R, protect procedure value when multiple rules apply, and shorten the time between surgery and cash. That difference matters to any practice manager trying to control days in A/R, reduce rework, and stop high-value cases from aging for preventable reasons.
What Are Orthopedic Billing Services
Orthopedic billing services aren't generic outsourced billing. They're specialty-specific RCM operations built around the way orthopedic practices get paid. That means they have to understand surgery scheduling, pre-auth workflows, operative report review, implant and supply support, post-op global rules, and payer edits that hit common orthopedic code combinations.
In practical terms, these teams work every part of the revenue cycle with orthopedic logic. They don't just ask whether a claim was filed. They ask whether the diagnosis supports the procedure, whether the op note establishes laterality, whether the payer requires distinct documentation for multiple procedures, and whether the claim should have gone out with a modifier that prevents an avoidable denial.
Orthopedics is one of the worst specialties for denial exposure. Claim denial rates in orthopedics range from 25% to 35%, and top-performing specialized billing companies report the ability to reduce denials by up to 60% while pushing clean claim rates to over 98% (AnnexMed's orthopedic billing benchmark review). That's why specialty billing isn't a nice-to-have. For many groups, it's the difference between predictable cash flow and constant rework.
Why generalist billing struggles
Most generalist billers fail in orthopedics for three reasons.
- They code from the schedule, not the chart. Orthopedic reimbursement depends on operative detail. "Knee scope" is not a billable story.
- They miss orthopedic payer logic. NCCI edits, global packages, and multiple procedure rules hit this specialty hard.
- They treat denials as back-office cleanup. In orthopedics, denial prevention has to start before surgery, with authorization, documentation, and claim edits lined up correctly.
A practice manager should expect an orthopedic billing service to know common code families and where the risk lives. Arthroscopy, fracture care, total joints, sports medicine, pain procedures, DME coordination, imaging, and trauma all create different billing patterns.
Orthopedic billing works best when coders review what happened clinically, not just what was booked operationally.
If you're comparing specialty options, look for a partner whose orthopedic workflow is built around these nuances rather than one trying to stretch a multi-specialty template. A focused example is Happy Billing's orthopedic billing specialty page, which reflects the level of orthopedic-specific process design a serious vendor should be able to describe in detail.
What the service should own
A credible orthopedic billing service should be able to take responsibility for:
- Charge review: Matching CPT, ICD-10, HCPCS, and modifiers to the operative note and encounter details.
- Pre-submission edits: Catching laterality, global, bundling, and sequencing problems before the claim leaves the system.
- Denial management: Not just appeal writing, but denial root-cause analysis by payer, code set, provider, and location.
- A/R follow-up: Working unpaid and underpaid claims aggressively enough to protect cash velocity.
- Payer communication: Escalating orthopedic-specific denials with documentation that addresses the reason for rejection.
Value isn't "outsourcing billing." It's removing preventable leakage from a specialty where coding details change payment outcomes.
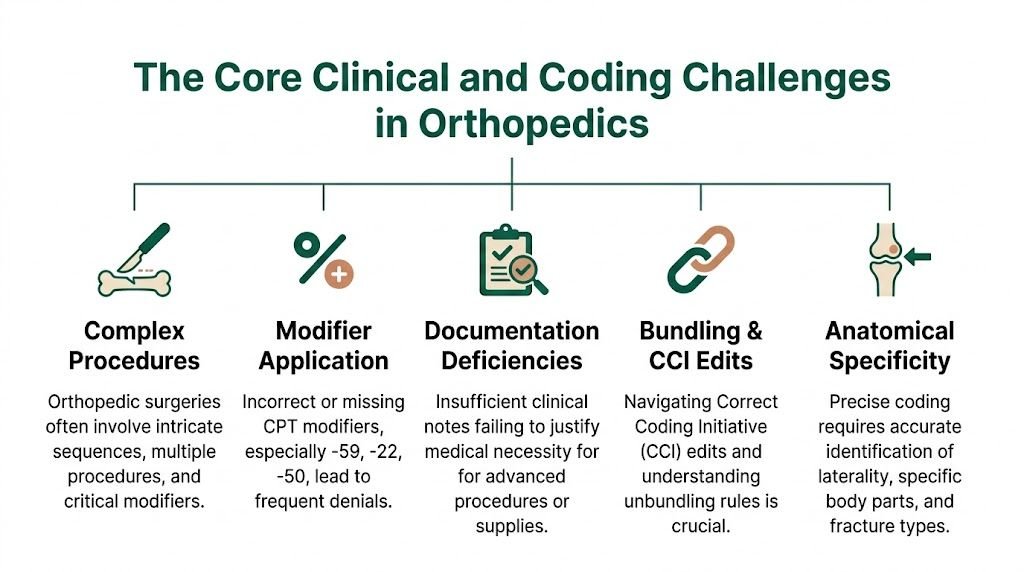
The Core Clinical and Coding Challenges in Orthopedics
Orthopedic reimbursement breaks down when the billing team doesn't think like a surgeon, coder, and payer at the same time. The challenge isn't volume alone. It's the combination of surgical packages, modifier precision, anatomical specificity, and payer edits that can turn a well-documented procedure into a denial if one field is wrong.
Global periods change what you can bill
A lot of orthopedic revenue leakage starts with poor global-period control.
Global period: A payer-defined span after surgery when related follow-up care is included in the original reimbursement and usually can't be billed separately.
Take CPT 27447 for total knee arthroplasty. If the patient returns during the post-op global period and the group bills a related service as though it's separately payable, the payer may fold it into the original surgery. If the patient has an unplanned return to the operating room during that global period, the billing team has to understand when modifier 78 is required and how documentation must support that return as an OR event tied to the original surgery.
The same issue shows up in fracture care and post-op complication management. Practices that don't maintain a usable global tracker inside the PM or EHR system end up billing from memory. That's where avoidable denials start.
For groups trying to tighten this workflow, a practical reference is this guide to orthopedic billing global periods.
Modifier mistakes create instant denials
Modifier discipline is not optional in orthopedics. It's one of the first things payers evaluate because orthopedic coding depends heavily on side, site, distinctness, and procedural relationship.
Modifier errors are a leading cause of orthopedic denials. Forgetting LT or RT on procedures involving bilateral structures, or missing modifier 78 for an unplanned return to the OR within a 90-day global period, are common errors that trigger immediate payer rejections under NCCI logic (ADSC's orthopedic billing guide).
The issue isn't only whether a modifier appears. It's whether the documentation supports it.
Modifiers that need close review
- LT and RT for laterality on paired structures such as knees, shoulders, wrists, and ankles.
- 78 for an unplanned return to the OR during the global period.
- 59 when a service is distinct and documentation supports separate reporting.
- 51 when multiple procedures are reported in the same session and sequencing matters.
- 50 when payer policy requires bilateral reporting in that format rather than side-specific line items.
A common example is shoulder arthroscopy. If the surgeon performs debridement and another arthroscopic service in the same encounter, the coder has to evaluate whether the secondary code is separately reportable or bundled. Throwing 59 on the line without operative support is not orthopedic expertise. It's denial bait.
Bundling and NCCI edits hit common orthopedic code pairs
Orthopedic surgery routinely involves code combinations that look separate clinically but may not be separately payable administratively.
Examples worth watching:
- CPT 29822 with 29826
- CPT 29881 with 29877
- Arthroscopy plus open repair combinations
- Primary procedure plus imaging guidance or supply line items that may be included depending on payer rules
The billing team has to review NCCI edit status, payer-specific bundling policy, and operative detail before submitting the claim. If the note doesn't describe a distinct site, separate lesion, different compartment, or separate surgical work that satisfies payer policy, the appeal usually fails later.
The fastest way to lose margin in orthopedics is to assume that every documented service is separately payable.
Documentation has to support coding, not just care
Orthopedic operative notes often describe excellent clinical care but still miss billing-critical details. For reimbursement, the note must usually make the anatomy, laterality, surgical approach, and medical necessity unmistakable.
A strong orthopedic note usually addresses:
- Anatomical specificity: exact joint, compartment, side, and structure treated
- Procedure detail: what was performed, not just the planned surgery
- Implant detail: when relevant, including the specific implant information documented in the record
- Complications and deviations: why added work or unexpected return procedures occurred
- Diagnosis linkage: how the post-op findings support the billed procedure set
If the surgeon documents "bilateral knee pain" but the claim is built around one side-specific procedure without clean side documentation, the claim editor may stop it immediately. If the op note describes additional repair work but doesn't clearly separate that work from the primary procedure, the coder may not have enough support to defend a separate line.
Implants, HCPCS, and payer-specific rules complicate surgical billing
Orthopedic billing isn't limited to CPT. Many claims also depend on correct HCPCS usage, supply reporting, and payer-specific rules for implants, DME, casting, braces, and injections. Some payers require invoice support for certain items. Others package supplies into the surgical payment unless contract language says otherwise.
A vendor's orthopedic expertise often becomes evident through these questions. Ask how they handle implant documentation, HCPCS validation, and claims that require attachments. If the answer is vague, they probably rely too heavily on generic workflows.
KPIs You Must Track for Orthopedic Revenue Health
Orthopedic practices can't manage reimbursement by feel. They need a small set of metrics that expose whether denials are falling, whether claims are going out clean, and whether money is sitting too long in A/R.
The benchmark numbers matter. Healthy orthopedic practices should target A/R under 40 days and a Net Collection Rate above 95%, while specialized billing services commonly charge 4% to 8% of collections (Spry on orthopedic billing company pricing and benchmarks). If a vendor charges premium pricing but can't show movement on those measures, the contract isn't paying for itself.
Orthopedic RCM KPI Benchmarks
| KPI (Key Performance Indicator) | Industry Benchmark (Healthy Practice) | What It Measures |
|---|---|---|
| Days in A/R | Under 40 days | How quickly the practice converts billed charges into cash |
| Net Collection Rate | Above 95% | How much of the allowed reimbursement the practice actually collects |
| Clean Claim Rate | Best practice is a very high first-pass acceptance level | How many claims go out correctly the first time without rework |
| Denial Rate | Lower is better, monitored by payer and denial reason | How much revenue is being delayed or blocked by preventable issues |
What each metric tells you
A/R days tells you whether cash is moving. If A/R is drifting upward, start by checking unworked denials, missing documentation, payer lag, and whether surgical claims are being held for coder review too long.
Net Collection Rate tells you whether contractual reimbursement is being captured. If it's weak, the practice may be writing off underpayments, failing to appeal denials effectively, or missing patient balance workflows tied to surgery scheduling and insurance follow-up.
Clean Claim Rate is the operational quality score. In orthopedics, low clean-claim performance usually traces back to missing modifiers, diagnosis mismatch, authorization problems, or claim edits involving bundled procedure combinations.
What a good report should include
A useful orthopedic revenue dashboard should show:
- Denials by CPT family
- Denials by modifier issue
- A/R by payer and aging bucket
- Underpayments on high-value surgical claims
- Appeal outcomes by denial category
If your current vendor reports only total charges, payments, and collections, that isn't orthopedic RCM reporting. It's bookkeeping. A stronger framework for this is outlined in these medical billing KPIs to track.
Practical rule: Track metrics at the code and payer level, not just at the practice-total level. Orthopedic problems hide inside procedure mix.
How to Evaluate an Orthopedic Billing Vendor
Most billing vendors sound competent in the sales call. A key test is whether they can answer orthopedic questions without retreating into generic language about "end-to-end revenue cycle support."
Start by making them work at the claim level.

Questions that expose real specialty knowledge
Ask the vendor to walk through scenarios like these:
- Bundled arthroscopy claim: "How would you review and appeal a denied 29881 when the payer bundled it with 29877?"
- Global return to OR: "What documentation do you require before billing a post-op procedure with modifier 78?"
- Laterality controls: "How do you prevent missing LT or RT on knee and shoulder claims?"
- Multi-procedure sequencing: "Who decides when 51 or 59 is appropriate, and what documentation standard do you use?"
- Implant-related support: "How do you handle claims that need invoice or attachment support for orthopedic supplies or implants?"
- Out-of-network trauma: "Who owns accident billing coordination and payer follow-up when the case came through the ER and coverage is unclear?"
A specialist should answer with workflow, claim edits, and documentation standards. A generalist usually answers with software buzzwords.
Red flags you shouldn't ignore
The fastest way to identify a weak vendor is to listen for what they avoid.
| Red flag | Why it matters |
|---|---|
| They can't discuss common orthopedic CPT combinations | They probably rely on generic coders |
| They promise low fees but avoid KPI accountability | Cheap billing gets expensive when denials rise |
| They don't separate orthopedic reporting by provider, code, and payer | You won't know where leakage lives |
| They treat appeals as a standard queue | Orthopedic appeals often require op-note-based arguments |
| They don't ask about global periods, trauma, or workers' comp | They don't understand orthopedic revenue drivers |
A vendor should also be willing to show sample reporting. You want to see denial reasons tied to procedure categories, modifier errors, authorizations, and payer edits. If they won't show that level of detail before signature, expect disappointment after go-live.
What strong vendors do differently
Strong orthopedic billing services usually have:
- Specialty coding review before claim submission
- Payer-specific edit logic for common orthopedic procedures
- A documented process for old A/R and aged surgical balances
- Escalation paths for underpayments and medical necessity denials
- A clear ownership model between your front desk, surgery scheduler, coder, and A/R team
You can sharpen your screening process with these medical billing company red flags. Use them before you compare pricing. Orthopedic billing quality is easier to evaluate upfront than to repair later.
Understanding Pricing Models and Contract Terms
Orthopedic billing services usually price on a percentage-of-collections model. That structure can work well because it aligns the vendor with cash realization, but only if the contract defines collections clearly and avoids hidden exclusions.
The typical range for orthopedic billing services is 4% to 8% of monthly collections (Spry's orthopedic billing pricing overview). In this specialty, the higher end usually reflects more intensive coding review, denial prevention, analytics, and A/R work on difficult surgical claims.
Comparing common pricing models
| Model | Best use case | Main trade-off |
|---|---|---|
| Percentage of collections | Most orthopedic groups | Easy alignment, but definitions matter |
| Flat monthly fee | Stable, predictable claim volume | Can weaken incentive on difficult A/R |
| Hybrid model | Groups with heavy surgery and legacy A/R | More flexible, but contracts get complicated |
Percentage pricing sounds simple until you ask what counts as a collection. It should be clear whether the fee applies to insurance payments only, patient payments, recovered old A/R, refunds, recoupments, and claims worked before the vendor took over. If the contract doesn't define those categories, disputes usually show up within the first few months.
Contract terms worth negotiating
Review these points closely before signing:
- Term length: Avoid getting trapped in a long initial term if the vendor can't prove orthopedic performance quickly.
- Termination clause: Watch for notice periods and early termination penalties.
- Data ownership: Your practice should control payer files, reports, work queues, and exported data.
- Access rights: Make sure your group keeps administrator-level visibility inside the EHR and PM system.
- Old A/R scope: Spell out whether aged claims are included or billed separately.
- Reporting cadence: Monthly isn't enough if the vendor isn't also giving usable weekly operational insight.
If the contract is easy to sign and hard to exit, it's protecting the vendor more than the practice.
For a broader comparison of outsourced billing fee structures, this breakdown of medical billing outsourcing cost models is a useful reference.
Best Practices to Reduce Denials and Speed Up Cash Flow
Orthopedic denials don't start in the billing office. They start when scheduling, authorization, documentation, and coding operate as separate silos. The best-performing groups treat denial prevention as a clinical and operational workflow, not just an A/R function.
Out-of-network and trauma-related orthopedic claims are a prime example. These claims can see denial rates as high as 35% because of coordination failures, and specialized RCM firms report recovering over 92% of aged claims through dedicated appeals teams (Medical Billers and Coders on orthopedic hospital billing challenges). Generalist billing teams usually struggle here because the file often requires accident details, payer order verification, medical records support, and persistent follow-up across multiple responsible parties.
Tighten the front end before surgery
Front-end discipline prevents a surprising share of orthopedic denials.
- Verify coverage against the actual procedure plan. A scheduled surgery shouldn't move forward on a generic eligibility check alone.
- Confirm authorization detail. The approved procedure set needs to match the expected CPT scope as closely as payer policy allows.
- Capture injury and accident information early. Trauma, motor vehicle, and out-of-network cases get harder to untangle after the claim is denied.
- Flag global and post-op relationships in advance. This helps prevent duplicate or non-payable follow-up billing.
A surgery scheduler and biller should be speaking the same language. If the surgery schedule says "shoulder scope with repair" and the authorization file is vague, the coder inherits avoidable risk later.
Improve the operative note for payment use
A good orthopedic note supports patient care. A billable orthopedic note supports payment review. Those aren't always the same thing.
Ask surgeons to document:
- Exact laterality and anatomical site
- Separate compartments or structures when relevant
- Why additional work was medically necessary
- Whether a return to the OR was unplanned
- Implant or supply detail when payer support may be required
This matters most on arthroscopy, fracture work, revisions, and post-op complications. If the note leaves room for payer interpretation, the payer will usually interpret against separate payment.
Run denial management as prevention, not cleanup
Many practices still work denials in batches after they age. That's too late. Orthopedic denial management should start with same-week root-cause review.
A strong process looks like this:
- Classify denials by reason and code family.
- Separate technical denials from clinical-necessity denials.
- Push fixes upstream to registration, authorization, coding, or provider documentation.
- Route appeal writing to staff who can read operative notes and payer policy language.
The best orthopedic A/R teams don't just reopen denied claims. They stop the next version of the same denial from going out.
For trauma and out-of-network work, create a dedicated queue. Those claims need a different playbook from routine commercial follow-up because liability, workers' comp, facility coordination, and emergency presentation all affect reimbursement timing.
Your Smooth Transition Checklist
Switching orthopedic billing services can improve collections, but a sloppy transition can freeze cash for weeks. The handoff has to protect claims already in flight while giving the new team enough context to work payer issues correctly from day one.

Data and documents
Pull together the records the incoming team will need before access goes live.
- Payer contracts and fee schedules
- Provider credentialing details
- Tax IDs, NPIs, and location setup
- Current authorization workflows
- Carrier contact lists and portal access information
- Recent denial reports and aging reports
- Top orthopedic CPT and diagnosis patterns by provider
If these aren't organized, the new vendor spends the first weeks rediscovering your practice.
Systems and claim access
Orthopedic transitions fail when system access is delayed or incomplete. Set this up early.
- EHR and PM access: Give role-based access for coding, claim edits, payment posting review, and reporting.
- Clearinghouse connectivity: Make sure rejections don't disappear between vendors during the change.
- ERA and portal access: The new team needs direct visibility into remits and payer claim status.
- Attachment workflows: Confirm how op notes, invoices, and medical records will be sent when claims require support.
Team ownership and communication
Name one practice-side owner for the transition. Don't split authority across the administrator, office manager, and physicians without a final decision-maker.
Use a working checklist that includes:
| Transition area | What to confirm |
|---|---|
| Open claims | Who owns submissions already billed but unpaid |
| Old A/R | Whether the new vendor will work aged balances immediately |
| Denials | Which team handles appeals during the overlap period |
| Charge lag | How quickly new encounters move from chart to claim |
| Escalations | Who decides on payer disputes and write-off approvals |
The first month should include frequent operational reviews focused on unbilled encounters, front-end edits, and unpaid surgical claims. In orthopedics, transition stability comes from visibility, not optimism.
Frequently Asked Questions About Orthopedic Billing Services
Do orthopedic billing services need certified coders or is orthopedic experience enough
You need both. Orthopedic billing is too dependent on CPT, ICD-10, HCPCS, modifier logic, and payer edits to rely on experience alone. Ask whether the team follows CMS guidance, AAPC coding standards, and payer-specific policy updates, then ask who reviews operative reports for high-value surgical claims. If they can't explain that workflow clearly, credentials on paper won't save performance.
What's the most common sign that a practice has outgrown a general billing company
The biggest sign is repetitive denial rework on common orthopedic procedures. If your team keeps seeing issues around laterality, bundled arthroscopy lines, post-op claim edits, or return-to-OR billing, the problem usually isn't staff effort. It's lack of specialty design. Practices also outgrow general vendors when physicians stop trusting the coding on their operative cases.
Should a billing vendor handle old orthopedic A R or only new claims
A strong vendor should be able to do both, but not with the same workflow. Old A/R needs focused recovery rules, payer triage, and appeal prioritization. New claims need prevention, edit control, and coding accuracy. Keep those workstreams separate in reporting so you can see whether the vendor is improving current performance or only collecting on legacy balances.
How often should an orthopedic practice audit coding and denial trends
Regularly enough to catch patterns before they become habits. For most practices, that means routine internal review of high-risk surgical claims, modifier use, and payer denials tied to recurring CPT combinations. Orthopedics changes too quickly to rely on annual cleanup. Review should be ongoing, especially for arthroscopy, fracture care, total joints, and trauma cases.
If your orthopedic practice needs tighter claim control, cleaner coding, and faster A/R movement without changing systems, Happy Billing is built for high-stakes specialties where modifier accuracy, global period management, and denial prevention directly affect cash flow.