Mastering the 93017 cpt code: 2026 Guide
93017 cpt code is the billing code for the technical tracing portion only of a cardiovascular stress test. If your team bills it like a full stress test, or uses the global code when the service was split between a physician and facility, you create avoidable denials, slow payment, and unnecessary rework.
That is the situation many cardiology practice managers are dealing with right now. The test was performed, the physician documented appropriately, but the claim still stalls because the billing team did not separate 93017 from 93015, 93016, and 93018 correctly.
Decoding CPT Code 93017 for Cardiovascular Stress Tests
A common denial starts the same way. The stress test is performed in a hospital outpatient department, the physician submits the claim as if the practice owned the full service, and the payer rejects or downcodes it because the technical piece belonged to the facility. That mistake ties up payment on a service that should have cleared on first pass.
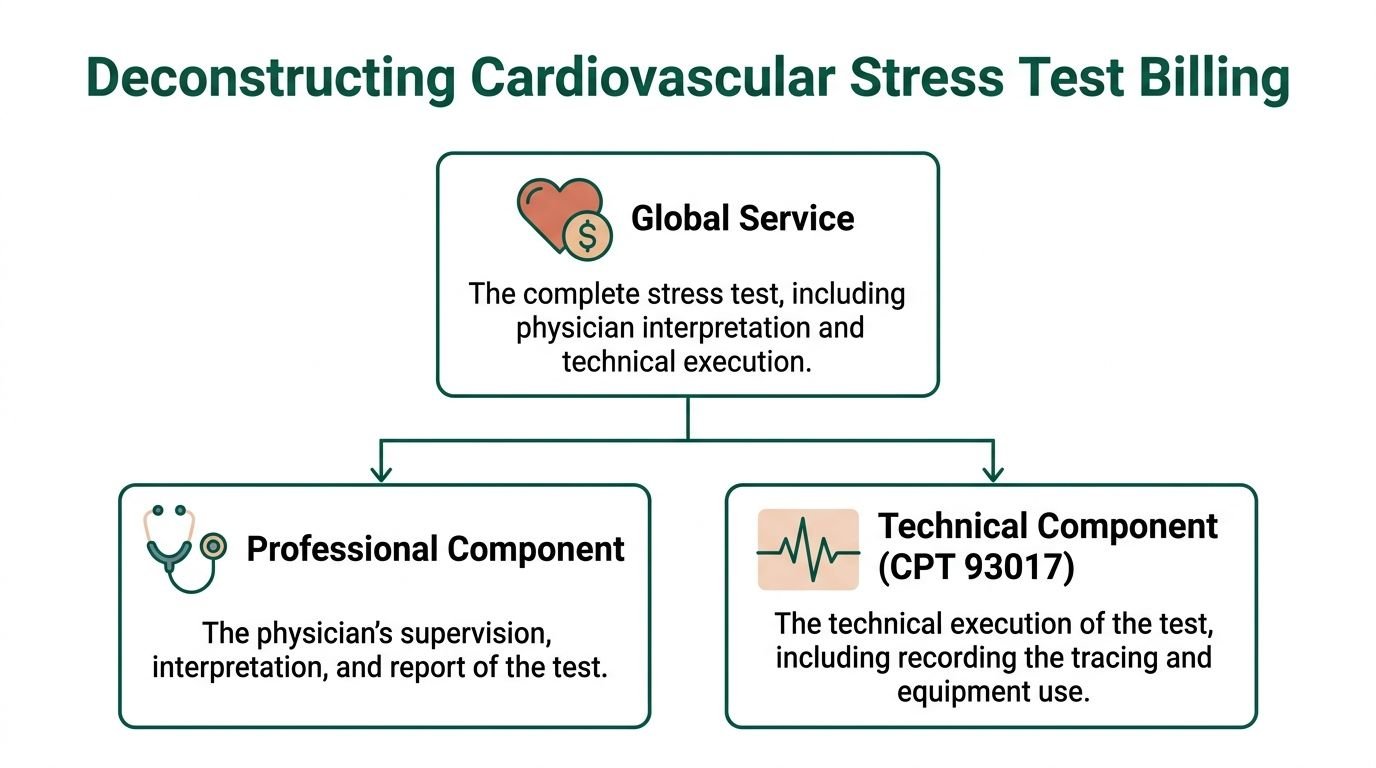
CPT 93017 reports the tracing only portion of a cardiovascular stress test. It represents the technical component, without physician interpretation and report.

What 93017 captures
For stress testing, 93017 applies to the ECG tracing and equipment-based portion of the service during maximal or submaximal treadmill exercise, bicycle exercise, and-or pharmacologic stress, without physician interpretation and report. It remains an active billable code in the Medicine, Cardiovascular category, and it appears on the Medicare Physician Fee Schedule. Reimbursement varies by payer, geography, and contract terms. A current coding and payment summary is outlined in this 93017 reimbursement and coding reference.
The revenue cycle point is simple. 93017 is an ownership code as much as a procedure code. If your practice did not provide the equipment, staff, and technical resources tied to the tracing, billing 93017 can create denials, post-payment recoupment risk, or both.
Why practice managers should care
Cardiology managers rarely lose sleep over the code description itself. They lose sleep over avoidable accounts receivable days, corrected claims, and repeat edits that keep the same dollars from posting.
The financial risk with 93017 is usually not undercoding. It is misallocated billing between the global service and separated components. A claim built with 93015 when the service was split can fail because the technical and professional portions were not owned by the same entity. A claim built with 93017 when documentation only supports physician supervision or interpretation can fail for the opposite reason.
That is why component separation matters operationally:
- Equipment ownership drives the technical claim. If the hospital or facility supplied the equipment and technical staff, that entity generally bills the tracing portion.
- Physician work must stand on its own code selection. Supervision and final interpretation are distinct professional services, not substitutes for 93017.
- Wrong component logic slows cash conversion. Staff then spend time on corrected claims, appeal work, and payment reconciliation instead of clean claim production.
Key takeaway: 93017 should trigger an ownership review before claim submission. Confirm who performed the technical tracing, who supervised the test, and who issued the interpretation report.
When 93017 is the right answer
Use 93017 when the billed service is limited to the technical tracing portion of the cardiovascular stress test and the record supports that technical work. The documentation should show the test setup, monitoring, data capture, and the practice or facility resources used to perform that portion of the service.
From an RCM standpoint, the question is not whether a stress test occurred. The question is which entity owned each billable component. Teams that build that check into charge review usually see fewer preventable denials and faster payment on stress test claims.
Understanding CPT 93017 and Its Component Counterparts
A cardiology practice can perform a stress test correctly and still lose time in A/R if the wrong component code hits the claim. The billing question is not whether the test occurred. The billing question is which party performed, owned, and documented each billable piece.
The component structure that matters in claims
Stress test coding works best when staff treat the service as four separate billing paths, then confirm whether one entity completed all of them.
| Code | What it represents | Revenue implication |
|---|---|---|
| 93015 | Global cardiovascular stress test | Appropriate only when one entity performs and bills the full service in the correct setting |
| 93016 | Supervision only | Supports physician oversight, not tracing or final interpretation |
| 93017 | Tracing only | Supports the technical portion only |
| 93018 | Interpretation and report only | Supports the physician reading and written report |
This distinction drives payment speed. If a practice bills 93015 when the technical portion belonged to the facility, the claim often stops in edits or comes back for correction. If the practice bills 93017 when the record only supports physician supervision or interpretation, payment risk shifts to a different denial reason.
Where code selection breaks down
The common error is treating 93017 like a partial version of 93015. It is a separate component with separate documentation and ownership rules. That difference matters because payers do not correct component logic for the billing office. They deny, reduce, or route the claim to manual review.
A second problem starts after the wrong base code is chosen. Staff try to rescue the claim with modifiers. That rarely works. Modifier logic only helps when the underlying CPT selection is already accurate. If your team needs a refresher on claim separation, this guide to modifier 59 use for distinct procedural services gives useful context.
Revenue impact of using 93017 correctly
93017 belongs on the claim when the billing entity furnished the tracing portion only. It does not replace supervision. It does not replace interpretation. It does not stand in for a global stress test, even if the encounter feels administratively connected.
From an RCM standpoint, component separation affects three areas:
- Charge capture accuracy. Front-end staff need a clear rule for when the technical claim belongs to the practice versus the facility.
- Edit prevention. Clean component selection reduces avoidable payer edits tied to ownership conflicts and overlapping billing.
- Cash flow timing. Correct first-pass billing cuts rework, corrected claims, appeal activity, and payment posting delays.
A practical comparison for charge review
Use these questions before the claim drops:
Who supplied the equipment and technical staff?
That answer usually determines whether 93017 belongs on the practice claim.Did the physician perform supervision only or the final interpretation only?
If so, 93016 or 93018 may fit the record better than 93015.Does the documentation separate tracing from interpretation clearly enough for an auditor to follow it?
If not, coders are forced to guess, and guessed code selection usually becomes rework.
One review point matters more than the rest. Component ownership should be confirmed before coding, not after denial.
What supports clean billing
Practices with fewer stress test denials usually do three things well:
- Build charge capture rules around site of service and resource ownership
- Treat 93015 as appropriate only when the full service is clearly performed by one entity
- Require chart language that separates technical tracing, physician supervision, and final interpretation
Practices that create preventable denials usually do the opposite:
- Let coders infer ownership from scheduling patterns or past habits
- Bill 93017 because a stress test occurred, without confirming who performed the tracing
- Add modifiers to a claim built on the wrong base CPT code
That is the operational value of understanding the counterparts to 93017. Correct component separation protects revenue, shortens follow-up time, and keeps stress test billing from turning into corrected-claim work.
Essential Documentation for Compliant 93017 Claims
A 93017 claim is only as strong as the record behind it. Payers do not pay for assumptions. They pay for a clearly documented technical service.
For 93017, the chart must prove that the claim is for tracing only, not supervision and not interpretation. If the record reads like a blended service, your billing team has already lost its advantage.
What the record should show
For compliant 93017 billing, the documentation should support the technical execution of the stress test and the tracing phase. The record should include complete test data tied to the technical service, and the technical specifications cited in payer-facing billing guidance include a full continuous 12-lead ECG strip, a stress protocol to target heart rate, and logs of vital signs.
A practical documentation checklist looks like this:
- Continuous ECG tracing: The strip should be complete and retained in the record.
- Stress modality: Treadmill, bicycle, or pharmacologic stress should be identified.
- Technician monitoring notes: The chart should show active technical monitoring during the test.
- Vital sign capture: Heart rate and blood pressure logs should be present.
- Start and stop context: The chart should show the protocol used and the reason the test ended.
- Technical-only separation: The documentation should not blur into physician interpretation language if 93017 is being billed by itself.
What auditors look for first
Auditors usually start with one question. Did the record support a technical tracing service, or did the claim submit a component code without proof of the component?
That is where weak documentation causes denials. “Stress test performed” is too vague. “Tracing obtained” is still too vague. The claim needs chart detail that demonstrates equipment use, physiologic monitoring, and technical capture.
Tip: Standardize a technician template inside the EHR. Free-text variability creates coding ambiguity, and coding ambiguity becomes denial volume.
Documentation that pushes you into a different code
Some records accidentally describe a broader service than 93017.
Examples include:
- A full physician interpretation and report appearing in the same technical note
- Supervision details documented without separation from the tracing workflow
- A global-style summary that suggests all service elements were provided by one entity
When the chart supports more than tracing, the coding decision has to change. If the chart supports less than tracing, the claim should not go out at all.
An operational fix that reduces rework
Practices that bill stress testing well usually separate documentation by role.
The technician documents the technical portion. The supervising physician documents supervision if applicable. The interpreting physician documents the final report. That separation makes charge review cleaner and gives the billing team a defensible record.
Teams refining this workflow often pair chart templates with a denial prevention process. A useful operational reference is this guide to medical billing denial management workflows, especially for turning recurring documentation misses into front-end edits instead of back-end appeals.
A simple standard for your staff
If the note does not clearly answer these three points, hold the claim:
| Review point | Why it matters |
|---|---|
| Was there a technical tracing service? | Supports 93017 itself |
| Is the technical data complete? | Supports medical necessity and service validation |
| Is physician interpretation excluded from this claim line? | Prevents code overlap and bundling risk |
Weak stress test billing is rarely caused by a lack of work performed. It is usually caused by poor separation between the work performed and the work billed.
Navigating Modifiers and NCCI Edits for 93017
Modifier mistakes on 93017 are often a symptom of a deeper problem. The team is trying to fix a component-code issue with a claims-processing tool.
That approach fails because 93017 is already a technical code. If the base code is wrong, modifier logic will not save the claim.

Modifier logic that billing teams should keep straight
The first rule is straightforward. Do not append TC reflexively to 93017. It is the technical component.
Verified billing guidance also notes that no TC modifier is needed for 93017 because the code itself already represents the technical service. Standard cases generally require no modifier (though PO may apply in off-campus provider-based settings). In facility settings, some workflows involve -26 on the professional side when physician-only services are billed, and the technical and professional components are split.
If your team needs a clean refresher on component modifiers, review modifier 26 versus TC in facility and non-facility billing. That distinction matters most when staff are deciding who owns which piece of the stress test.
The NCCI edit that causes the most preventable denials
The major trap is billing 93017 with 93015. That pairing creates a bundling conflict because 93015 is the global service and already includes the component work.
Another verified rule is equally important. Do not bill 93017 with 93018 when the overlap would create a component conflict based on payer edit logic. The cleaner approach is to split codes according to who performed and owned each part of the service.
According to this 93017 RCM and edit analysis, 93017 should be rigorously unbundled from the professional components, and bundling edits involving 93017 with 93015 or 93018 can drive 20-30% rejection rates, while misuse of 93015 in hospital settings can lead to 100% denial when the service must be split into components. The same source notes that accurate component billing supports 98%+ clean claim rates, with technical documentation including a full ECG strip, stress protocol details, and vital-sign logging.
Place of service changes the billing logic
Many practices lose money without realizing it here.
In a non-facility physician office setting, the practice may own and perform the entire service and can evaluate whether global billing is appropriate. In a facility setting, such as hospital outpatient, the technical portion is typically separated. The facility bills the technical service, and the physician bills only the professional component furnished.
That means your charge capture should not start with code preference. It should start with place of service and ownership.
A workable edit strategy
Use your claim scrubber and PM system to enforce a few hard stops:
- Block 93017 + 93015 on the same date for the same encounter
- Review 93017 + 93018 combinations for overlap
- Reject multiple units of 93017
- Check site-of-service logic before releasing any global stress test claim
- Require documentation of technical tracing elements before 93017 drops to claim
Best practice: Put the site-of-service check before coder review, not after. Once a claim is built as global, staff are more likely to “fix” it with modifiers instead of rebuilding it correctly.
Pairing with other services
Verified guidance indicates that 93017 + 93350 can be billed together in a valid stress echo scenario when documentation and medical necessity support both services. The point is not to bundle everything apart. The point is to separate only what must be separated.
The same source also notes that ICD-10 validation is part of the workflow, including CMS-listed options such as R94.31 for abnormal ECG, and diagnosis families like I20-I25 when clinically appropriate. Those diagnosis choices are not just coding details. They determine whether the technical tracing claim has a medically necessary reason to exist.
When teams understand NCCI edits and site-of-service rules together, denials fall for a simple reason. The claim matches the service structure.
Sample Claim Lines and 93017 Reimbursement Rates
The cleanest way to understand 93017 is to look at it like a claim scrubber would.
A valid 93017 claim line should show a technical tracing-only service, a medically appropriate diagnosis, one unit, and no unnecessary modifier when the code already represents the technical component.
Example of a clean claim line
Here is a simple example for a technically performed cardiovascular stress tracing claim:
| CPT/HCPCS | Modifier | Units | Diagnosis pointer | Claim note |
|---|---|---|---|---|
| 93017 | none in a standard tracing-only scenario | 1 | I20.9 | Technical component only, tracing without interpretation/report |
That diagnosis example is practical because verified billing guidance specifically notes that 93017 is commonly paired with CMS-listed ICD-10 families such as I20-I25, for coronary artery disease and related stress-test indications, as described in this 93017 coding and reimbursement guide.
What not to put on the claim
Do not create a claim line that implies the physician interpreted the study when you are billing 93017 only.
Avoid:
- Adding a redundant TC modifier by habit
- Billing more than one unit
- Pairing the tracing-only claim with same-day 93015 for the same service
- Releasing the claim if the technical note does not clearly support tracing-only performance
2026 estimated reimbursement for CPT 93017
The reimbursement range available in the verified data is narrow enough to be useful for budgeting and contract comparison.
| Payer | National Average Rate (Facility/Non-Facility) | Notes |
|---|---|---|
| Major payers range | $56.25 to $76.59 | 2026 national average range reported in verified billing references |
| Medicare average | $62.01 | Reported in verified billing guidance focused on 93017 reimbursement |
| Private payer example average | $76.59 | Reported in verified billing guidance as a benchmark |
These are 2026 estimated reimbursement figures reported in billing references verified in October 2025, and actual payment still varies by locality, payer contract, and MAC.
How practice managers should use the rate data
Do not use these numbers as a static expectation for every claim. Use them as a benchmark.
A better use case is internal:
- Compare actual allowed amounts against your payer mix
- Monitor whether facility versus non-facility billing patterns are consistent
- Identify underpayments where the code selection was correct but reimbursement did not match contract terms
For teams trying to connect coding quality to cash flow, this overview of cardiology revenue cycle management is useful because stress test component coding is one of the places where operational discipline directly affects net collections.
Key takeaway: The value of 93017 is not just the fee. The larger revenue impact comes from preventing the rebill cycle that starts when the claim is filed as the wrong component.
Preventing Common Denials for CPT Code 93017
Most 93017 denials are not random payer behavior. They come from repeatable process failures inside registration, charge capture, documentation, and claim scrubbing.
That is good news for a practice manager, because repeatable failures can be fixed.

Denial pattern one, component overlap
The most expensive denial pattern is still the simplest. The claim treats a component code like a global service or bills overlapping services together.
When staff submit 93017 with global or conflicting component logic, the payer edit usually catches it immediately. The fix is not an appeal template. The fix is a front-end hard edit.
What works
- A charge rule that blocks same-day overlap with incompatible stress-test coding
- Separate charge pathways for physician office and hospital outpatient workflows
- Coder review triggered by any mixed technical and professional language in the chart
Denial pattern two, wrong place of service logic
A second denial pattern comes from billing the right code in the wrong site-of-service framework.
This usually happens when a practice uses office logic for hospital work. The physician practice submits a service as though it owned the technical piece, but the facility performed it. The payer sees the mismatch before the claim is paid.
A practical prevention workflow
- Registration confirms the site of service at scheduling.
- Charge capture maps the encounter to facility or non-facility logic.
- The claim scrubber blocks global stress test billing when the encounter indicates facility ownership.
- Billing staff review only exceptions, not every routine claim.
Denial pattern three, documentation that fails the tracing-only standard
A 93017 claim can also fail because the chart does not prove the technical service cleanly enough. If the technical note is sparse, missing key test data, or reads like a partial professional report, the payer has room to deny.
That is why technician templates matter. They reduce variation and make claims easier to defend.
Denial pattern four, weak diagnosis linkage
Even technically perfect claims fail when the diagnosis pairing is weak or unsupported.
The billing team should not guess. The diagnosis attached to 93017 must support why a cardiovascular stress tracing was medically necessary. Practices that struggle here usually need a pre-bill diagnosis validation rule tied to their stress test workflow.
The operating model that prevents leakage
Strong 93017 performance comes from process design, not heroics.
A reliable workflow usually includes:
- Scheduling checks: Confirm payer requirements and setting before the test
- Role-based documentation: Technician, supervising physician, and interpreting physician document separately
- Charge review logic: Build edits around ownership and component separation
- Pre-claim scrubbing: Stop conflicting code combinations before submission
- Denial feedback loop: Turn every avoidable denial into a new front-end edit
For teams dealing with recurring cardiovascular claim failures, this resource on cardiology billing denials is a practical reference. Practices that want outside support for this part of the revenue cycle often look to specialized cardiology billing services when in-house staff are spending too much time correcting the same stress-test mistakes.
Operational truth: Every corrected 93017 claim costs more than preventing the error upstream. The best denial management strategy is fewer denials entering the system in the first place.
Frequently Asked Questions About CPT 93017
Can CPT 93017 be billed with 93015
No. 93015 is the global cardiovascular stress test service, so billing it with 93017 for the same service creates component overlap and usually triggers a bundling denial. If the service was split, bill the individual component codes that match the work performed and the entity that performed it.
Does CPT 93017 need modifier TC
Usually no. 93017 is already the technical component code, so appending TC is generally redundant in standard cases. Modifier use should follow the billing context, and teams should be especially careful not to use modifiers as a workaround for incorrect base-code selection.
Can 93017 be billed in a hospital setting
Yes, but it must follow facility billing logic. In hospital outpatient workflows, the technical component is generally separated from the physician work. That means the hospital commonly bills the tracing component, while the physician bills only the professional service furnished.
What documentation best supports a 93017 claim
The strongest record shows a clear tracing-only service. That includes the continuous ECG tracing, stress protocol details, technician monitoring, vital sign logs, and technical test data without blending the note into physician interpretation or report language.
If your stress test claims are getting delayed because the work performed, the documentation, and the code selection are not lining up, Happy Billing helps cardiology and other specialty practices tighten component coding, prevent denials before submission, and improve cash flow without forcing an EHR migration.