Mastering CPT Modifier 59 for Clean Claims in 2026
CPT Modifier 59 is used to identify a "Distinct Procedural Service," telling a payer that a procedure or service, normally bundled into another, was performed separately and warrants separate payment. Proper use requires appending it to a CPT code to bypass a National Correct Coding Initiative (NCCI) edit when a service is performed at a different session, on a separate anatomical site, or for a distinct injury. It should only be used as a "modifier of last resort" when a more specific X-modifier (XE, XS, XP, XU) does not accurately describe the clinical scenario.
It’s meant to bypass a National Correct Coding Initiative (NCCI) edit, but only under very specific circumstances: a different patient session, a separate anatomical site, or a distinct injury. Think of it as your last resort—the modifier you reach for only when a more specific one (like XE, XS, XP, or XU) just doesn't fit the clinical story.
Understanding When to Use CPT Modifier 59
Using Modifier 59 correctly is all about clear communication with payers. Its job is to unbundle two services that are normally packaged together, but only when the clinical situation makes them genuinely separate. When you append Modifier 59, you’re attesting that the service wasn't just a component of another procedure but was a distinct, necessary service on its own.
The entire game hinges on what makes a service “distinct.” The Centers for Medicare & Medicaid Services (CMS) has laid out clear ground rules. If your scenario isn't on this list, using the modifier is a major compliance risk.
Scenarios Justifying Modifier 59
- Different Session or Patient Encounter: A service performed in the morning is clearly distinct from one performed later that same afternoon by the same provider.
- Different Procedure or Surgery: Two procedures that are fundamentally different in nature are performed on the same day.
- Different Site or Organ System: A procedure on the left knee is distinct from a procedure on the right shoulder. Simple as that.
- Separate Incision, Excision, Lesion, or Injury: Treating two different lesions on a patient's back, where each requires its own separate incision and closure, would qualify.
Think of it this way: NCCI edits assume you ordered the combo meal (bundled services). Modifier 59 is you telling the payer, “No, we ordered the fries and the drink separately for a specific reason,” justifying two distinct charges.
Getting this right is absolutely critical for a healthy revenue cycle. Proper use ensures you’re paid for all the work you actually performed, preventing the kind of automatic denials that crush cash flow. As our guide on what defines a clean claim in medical billing explains, accurate coding is the backbone of first-pass payment rates.
There's a reason Modifier 59 is under so much scrutiny. Created by the American Medical Association in 1994, it became so overused that by the mid-2010s, CMS had flagged it as a massive compliance problem. According to one Medicare Administrative Contractor, it’s still the most-used modifier among Part B providers, instantly raising red flags for auditors looking for fraud and abuse. The full story of why the modifier is considered overused is a must-read for any billing department. This rampant misuse creates headaches for practices in every specialty, making correct application non-negotiable.
Choosing Between Modifier 59 and the X-Modifiers
If your team is still defaulting to CPT Modifier 59 to get claims paid, you’re operating with an outdated playbook—and practically inviting denials. While it was once the go-to tool for bypassing NCCI edits, its chronic overuse has put it directly in the crosshairs of payer audits.
Think of Modifier 59 as the master key for your billing department. Sure, it opens a lot of doors, but it also trips every single alarm on the way in. It’s non-specific, tells payers very little, and signals that your coders might not be digging deep enough into the clinical scenario.
The X-modifiers, on the other hand, are the precision tools. They’re like keys cut for individual locks, telling a payer not just that a service was distinct, but exactly how. Using them correctly is a non-negotiable best practice for any practice serious about clean claims and avoiding audits.
This decision path shows exactly when to reach for a specific X-modifier instead of the broad Modifier 59.
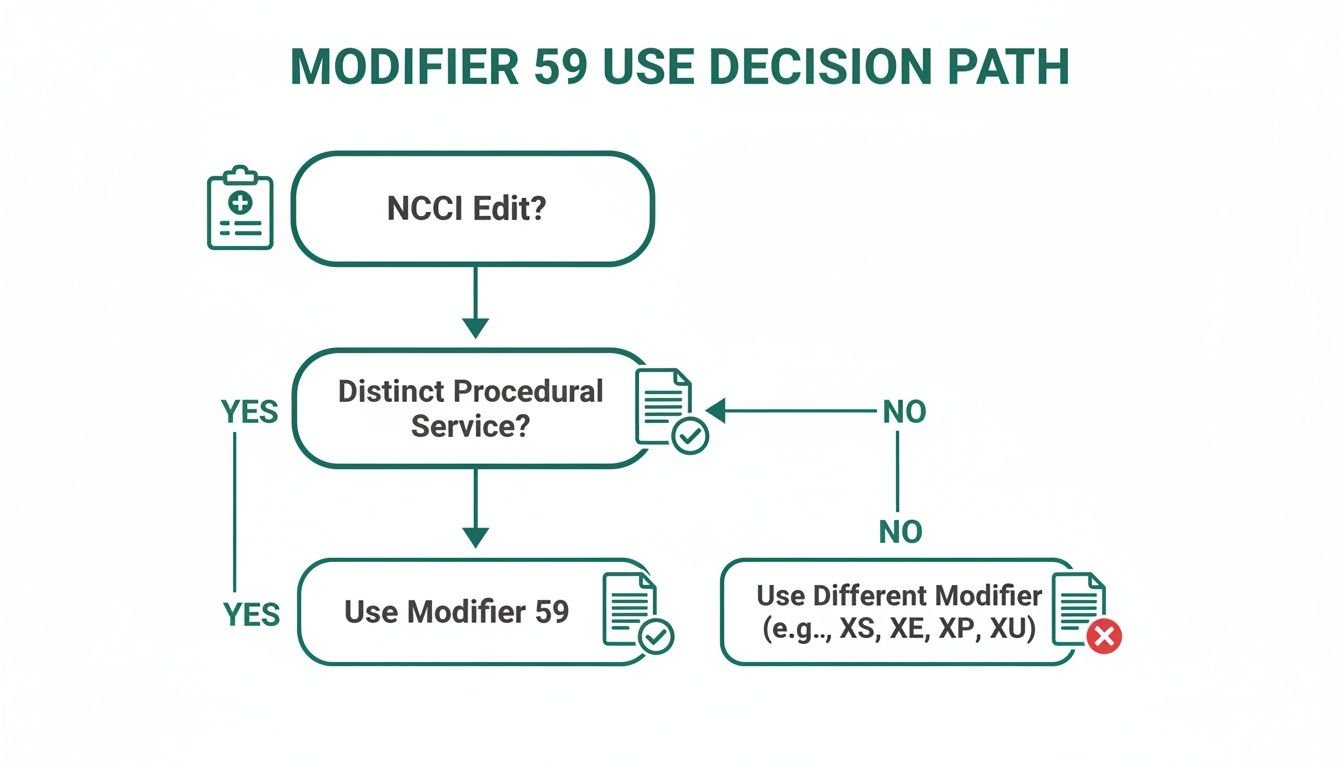
The moment your team hits an NCCI edit, a new question should pop up: "Does an X-modifier fit this scenario?" Only after you’ve ruled them all out should you even consider using Modifier 59.
To make this choice crystal clear, here’s a quick guide for selecting the right modifier. Always aim for the most specific option available before falling back on the general Modifier 59.
Choosing the Right Modifier to Bypass NCCI Edits
| Modifier | Name | When to Use | Example Scenario |
|---|---|---|---|
| XE | Separate Encounter | A service that is distinct because it occurred during a separate session on the same day. | Patient has a procedure in the morning, then returns to the same clinic in the afternoon for a completely separate, unplanned service. |
| XS | Separate Structure | A service that is distinct because it was performed on a separate organ or a different anatomical site. | A dermatologist removes a lesion from the patient's arm and, in the same visit, biopsies a suspicious mole on their back. |
| XP | Separate Practitioner | A service that is distinct because it was performed by a different clinician in the same group practice. | One physician in your group performs a test, and a different partner provides the interpretation and report later that day. |
| XU | Unusual Non-Overlapping Service | A service that is distinct because it doesn’t typically overlap with the main procedure’s components. | During a diagnostic procedure, an unexpected finding requires a separate, distinct therapeutic intervention that isn’t normally part of the diagnostic scope. |
| 59 | Distinct Procedural Service | The “modifier of last resort” used only when no other, more specific modifier (like XE, XS, XP, or XU) is appropriate. | Used to unbundle services that are truly distinct but don't fit the "eXact" definitions of the X-modifiers. Its use requires robust documentation. |
The takeaway is simple: specificity wins. Using the X-modifiers shows payers you’ve done your homework and provides the justification they need to process the claim without a manual review.
Why the X-Modifiers Even Exist
The X-modifier family wasn’t created on a whim. CMS introduced them back in 2015 through Change Request 8863 to combat the rampant misuse and abuse of Modifier 59. The goal was to force billing departments to get more specific about why a service was truly separate.
But here’s the problem: adoption has been slow. Many practices still lean on Modifier 59 as a crutch, which is a major red flag for savvy payers in 2026. While CMS still technically allows it, choosing 59 when an X-modifier is more appropriate signals outdated billing habits and puts a target on your back.
Let's break down the "X-Factor" family:
XE – Separate Encounter: Use this when a service happens in a completely different session on the same day. For example, a patient gets a therapeutic injection (CPT 20610) in the morning and comes back in the afternoon for an unrelated debridement (CPT 11042). Appending XE to the second procedure tells the story perfectly: two visits, two distinct services.
XS – Separate Structure: This is your go-to for procedures on different organs or anatomical sites. Imagine a dermatologist excises a lesion from the back (CPT 11602) and also biopsies a suspicious spot on the arm (CPT 11102). You’d append modifier XS to 11102 to show it was performed on a completely different body part.
XP – Separate Practitioner: This modifier clarifies that two different doctors in your practice delivered services on the same day. For instance, one cardiologist reads an EKG (CPT 93010) in the morning, and their partner handles a follow-up consultation later that afternoon. XP makes it clear two different providers were involved.
XU – Unusual Non-Overlapping Service: This one is the most nuanced. Think of it as the modifier for when a procedure is distinct because it uses none of the components of another service performed at the same time. A classic example is when a diagnostic endoscopy unexpectedly leads to a surgical procedure that isn't typically bundled with the initial scope. XU explains that the second service was truly separate and unusual.
Switching to an "X-modifier first" mentality is a powerful, proactive strategy. It provides payers with the precise justification they need upfront, drastically reducing your audit profile and denial rate.
If your practice is also wrestling with unbundling issues around evaluation and management services, check out our guide on CPT Modifier 25. Implementing a more granular approach across the board is the key to optimizing your entire revenue cycle.
How to Navigate NCCI Edits and Payer Rules
Modifier 59 exists to fix one major headache for your practice: The National Correct Coding Initiative (NCCI) and its automated Procedure-to-Procedure (PTP) edits. These are the built-in rules that let payers automatically bundle related services into a single payment, assuming one procedure was just part of another.
Properly using CPT modifier 59 is how you challenge that assumption and get paid for all the distinct work you actually performed.
Think of NCCI edits as a default setting. When certain CPT codes are billed together, the payer’s system assumes one is just a smaller component of the other. The edits are laid out in two columns: a Column 1 code (the main procedure) and a Column 2 code (the lesser procedure that gets bundled). Bill both without a modifier, and the Column 2 code is automatically denied.
Understanding the Correct Coding Modifier Indicator
So how do you know if you can even fight the bundling edit? The answer is in the Correct Coding Modifier Indicator (CCMI), a simple number CMS publishes in the NCCI tables. This little flag tells you everything you need to know.
CCMI of '0': This is a hard stop. A '0' means the codes are permanently bundled and can never be billed separately. Slapping a Modifier 59 on this claim is a guaranteed denial. The services are considered integral to each other, no exceptions.
CCMI of '1': This is your green light. A '1' signals that you can use a modifier (like 59 or a more specific X-modifier) to bypass the edit—if your clinical documentation proves the services were truly separate and distinct.
CCMI of '9': This is rare, but it means the edit was deleted. You don't need a modifier because there's no longer a bundling rule in place.
Getting these rules right is the foundation of preventing unnecessary write-offs. Our team lives and breathes this stuff, turning complex payer logic into predictable cash flow. You can see how we stop these issues before they start by checking out our guide on effective medical billing denial management.
A Real-World NCCI Edit Example
Let’s make this real. Here’s a classic scenario in wound care or dermatology. Your provider performs a subcutaneous tissue debridement and applies a skin substitute graft during the same patient encounter.
- Column 1 Code: CPT 15271 (Application of skin substitute graft to trunk, arms, legs, first 25 sq cm or less)
- Column 2 Code: CPT 11042 (Debridement, subcutaneous tissue; first 20 sq cm or less)
The NCCI tables pair these codes with a CCMI of '1'. Without a modifier, the payer will deny the debridement (11042) as a simple, included part of the skin graft application (15271).
Key Takeaway: The payer’s default assumption is that any debridement at the same site is just necessary prep work for the graft and is already baked into the graft’s reimbursement.
But what if the debridement was performed on a completely different wound? Say, the graft was applied to the left leg, but the debridement was for a separate ulcer on the right arm.
Now it’s a distinct procedural service. In this case, you would append Modifier 59 (or, even better, the more specific modifier XS for "Separate Structure") to the debridement code: CPT 11042-XS.
This simple addition tells the payer that the debridement wasn’t prep work for the graft—it was a medically necessary procedure on a different body part entirely. By checking the NCCI tables first and applying the right modifier, you turn a certain denial into a clean, first-pass payment.
Real-World Examples for Applying Modifier 59
Seeing CPT Modifier 59 in action is the only way to truly get it right. These specialty-specific scenarios show you exactly how to justify a distinct service, bypass an NCCI edit, and secure the reimbursement you've earned. Think of these as your claim-level blueprints for turning complex clinical situations into clean, paid claims.
The one thing all these examples have in common? Documentation. Without a medical record that paints a crystal-clear picture of two separate services, even the most perfect use of Modifier 59 will end in a denial.
Dermatology Destruction and Biopsy
Dermatology practices live and breathe this stuff. Performing multiple procedures on different lesions in one visit is a daily occurrence, making it a classic scenario where Modifier 59—or better yet, an X-modifier—is absolutely essential.
Picture this: a patient comes in with two problems. They have a benign keratosis on their left cheek and a suspicious-looking nevus on their right shoulder. The dermatologist decides to destroy the keratosis and take a biopsy of the nevus.
- Procedure 1: Destruction of a benign lesion (CPT 17000) on the left cheek.
- Procedure 2: Tangential biopsy of a single lesion (CPT 11102) on the right shoulder.
The NCCI edit bundles the biopsy (11102) into the destruction code (17000). If you bill them without a modifier, the biopsy will be denied. The fix is to append a modifier to the biopsy code, signaling it was performed on a completely separate anatomical site.
Correct Billing:
- Line 1: 17000
- Line 2: 11102-XS
In this case, Modifier XS (Separate Structure) is the best choice. It tells the payer exactly why the service was distinct: different anatomical location (shoulder vs. cheek). If you're dealing with a payer that doesn't recognize X-modifiers yet, you would fall back on CPT Modifier 59 (11102-59), but your documentation must spell out the two separate sites.
Orthopedics Surgery and Injection
Orthopedics is another specialty where multiple procedures in different anatomical areas are the norm. This scenario is particularly relevant for practices looking to tighten up their revenue cycle, and it's an area where Happy Billing offers deep expertise in orthopedics billing and coding.
Let's say a patient has a scheduled arthroscopic meniscectomy on their right knee. During that same trip to the OR, the surgeon also gives them a corticosteroid injection in their left shoulder to treat a separate, pre-existing case of bursitis.
- Procedure 1: Arthroscopy, knee, surgical; medial or lateral meniscectomy (CPT 29881).
- Procedure 2: Injection of a major joint (e.g., shoulder); (CPT 20610).
NCCI edits bundle that injection (20610) right into the arthroscopy (29881). Billing them together without a modifier makes it look like the injection was part of the knee surgery—like a post-op pain block—and it will be denied instantly.
To get paid, you have to use a modifier to prove the injection was for a totally different body part.
- Correct Billing: CPT 29881, CPT 20610-XS (or 20610-59)
- Essential Documentation: The operative note must clearly describe the knee arthroscopy and then, in a separate section, document the medical necessity and procedure for the left shoulder injection. No ambiguity allowed.
Physical Therapy Timed Codes
Modifier 59 gets especially tricky with timed CPT codes, creating major compliance headaches for specialties like physical therapy. Here, the rule is that two distinct services must be performed in separate, non-overlapping blocks of time. This is a documentation nightmare that trips up countless practices, leading to high denial rates and audit flags.
For any practice that depends on time-based billing, like anesthesiology or mental health clinics, getting this wrong can stall reimbursement and wreck cash flow. You can read the full analysis on modifier compliance for timed codes to see just how critical expertise is here.
Here’s a common physical therapy example. A therapist provides two distinct 15-minute services in one session.
- Service 1: Manual therapy techniques (CPT 97140) for 15 minutes to mobilize the patient's thoracic spine.
- Service 2: Therapeutic activities (CPT 97530) for 15 minutes to improve balance and coordination on an obstacle course.
NCCI pairs CPT 97140 and CPT 97530. To get paid for both, you must prove they were performed back-to-back, not at the same time.
Correct Billing & Documentation:
- Append Modifier 59 to CPT 97530 (the secondary code).
- Your documentation must have time stamps. For example: "9:00–9:15 AM: Manual therapy to T-spine. 9:15–9:30 AM: Therapeutic activities focused on dynamic balance."
Without that time-stamped proof, the payer will assume the services overlapped and deny one. For time-based codes, this level of detail is absolutely non-negotiable.
Documentation That Justifies Modifier 59 Usage
Using CPT modifier 59 isn’t just a coding choice—it's a statement. You're telling the payer that a service was distinct and medically necessary, and you're essentially daring them to check your work.
When auditors from CMS and commercial payers inevitably come knocking, your clinical documentation is your only line of defense. Without it, even a perfectly appropriate modifier will get you a denial.
Your goal is to paint a picture so vivid that an auditor understands the clinical story at a glance. The notes need to answer the payer's questions before they're even asked, leaving zero room for an auditor to misinterpret the encounter.
The Blueprint for Bulletproof Notes
To justify bypassing an NCCI edit, your documentation has to contain specific, non-negotiable details. Vague notes and boilerplate language are a fast track to a failed audit and lost revenue.
Auditors are trained to hunt for these core elements. Make their job easy.
Distinct Anatomical Sites: Don’t just say "arm" or "leg." Be hyper-specific. Think "left forearm, 2cm proximal to the wrist" versus "right antecubital fossa." For anything paired, call it out: "left kidney" vs. "right kidney," or "second digit, right hand" vs. "third digit, left foot."
Separate Sessions or Encounters: If services happened at different times on the same day, your notes absolutely must include time stamps. For example: "9:15 AM: Wound debridement of sacral ulcer completed. 1:30 PM: Patient developed acute respiratory distress, requiring a separate, unplanned nebulizer treatment."
Separate Incisions or Lesions: For dermatology and surgery, every lesion or incision gets its own story. Document the precise location, size, and medical necessity for each procedure separately. For instance: "Lesion A (left shoulder) was biopsied due to…" followed by a separate entry for "Lesion B (right cheek) was destroyed via cryosurgery because…"
Embedding Compliance into Your EMR
The single best way to get consistent, compliant documentation is to build it right into your EMR. Stop relying on providers to remember every detail under pressure and start using structured templates.
Key Insight: Proactive documentation is your best defense against audits. By embedding specific language into your EMR templates, you force the narrative to be compliant from the moment the note is written, turning documentation from a chore into a powerful revenue protection tool.
Add specific fields or dropdowns for laterality (Left, Right, Bilateral), anatomical specifiers, and session times. You can even embed sentence starters into your note templates to guide providers toward compliance. Imagine a post-procedure note that includes a mandatory prompt:
"Following the completion of the [Primary Procedure], a separate and distinct clinical decision was made to perform [Secondary Procedure] because…"
This simple addition forces the clinician to document their rationale, instantly creating an audit-proof record. Mastering documentation isn't just about ticking compliance boxes; it's about building a fortress around your revenue. For high-volume specialties like dermatology, a single audit can be devastating—learn how to get ready by reviewing our guide to the dermatology modifier 25 audit process.
How We Stop Modifier 59 Denials Before They Start
Wrestling with CPT Modifier 59 in-house is a constant drain on your practice. It leads to a cycle of frustrating denials that choke your cash flow and eat up staff time. We don’t just manage those denials—we make sure they never happen in the first place.
Our entire process is built on getting your claims right the first time. We combine a proprietary, AI-powered claim scrubber with a final review by our own AAPC-certified coding experts. This one-two punch is designed to guarantee modifier accuracy on every single claim that leaves your practice.
Our Two-Stage Validation Process
The second a claim is created, our system gets to work. It instantly cross-references the claim against a massive database of rules, including all NCCI edits and thousands of specific commercial payer policies. Any claim with a potential Modifier 59 or X-modifier error is flagged immediately.
This isn't about waiting for a rejection letter. Our system catches the mistakes that cause most modifier denials in seconds, right at the source. This proactive scrubbing is the key.
But we don't just let the computer fix it. Once a claim is flagged, it’s escalated to our team of human coding specialists. They dig into the clinical documentation to confirm what’s really going on and decide on the right fix. They will:
- Correct the modifier to the most specific one available (like swapping a generic 59 for a more precise XS).
- Append the correct modifier if it was missed entirely.
- Work directly with your team to get the documentation needed to back up the modifier and secure payment.
This two-stage validation is exactly how we hit our 98%+ first-pass clean claim rate. It breaks the costly cycle of denials and appeals that plagues so many practices. We turn your revenue cycle from a source of frustration into a predictable engine for growth.
By taking these complexities off your plate, we free up small practices to get back to patient care, not paperwork. You can learn more about how we help practices like yours in our guide to medical billing for small practices.
Can I Use Modifier 59 on an E/M Service Code?
No. Modifier 59 must never be appended to an Evaluation and Management (E/M) code (e.g., CPT codes 99202-99215). According to both CMS and AAPC guidelines, this modifier is exclusively for unbundling procedural services. If a physician performs a significant, separately identifiable E/M service on the same day as a procedure, the correct modifier to append to the E/M code is Modifier 25. Using Modifier 59 on an E/M code is a fundamental error that guarantees a denial.
What Is the Top Reason for Modifier 59 Denials?
The primary driver of Modifier 59 denials is insufficient documentation. Payers and auditors require the medical record to explicitly justify why the service was distinct. This means clearly noting separate anatomical sites (e.g., "left arm" vs. "right leg"), separate patient encounters (with timestamps), or separate incisions. Another common reason for denials in 2026 is using the general Modifier 59 when a more specific X-modifier (like XE, XS, XP, or XU) would have been more appropriate for payers that recognize them.
Does Modifier 59 Prevent Payment Reductions?
No. Modifier 59's sole function is to bypass an NCCI PTP edit to allow a bundled service to be considered for separate payment. It does not protect against the Multiple Procedure Payment Reduction (MPPR). Under MPPR rules, most payers will still reduce payment on the second and subsequent procedures performed during the same session—often by 50% of the standard fee schedule amount. Correctly using Modifier 59 gets the claim paid, but the MPPR determines how much it gets paid.
Should I Use X-Modifiers If a Payer Doesn’t Recognize Them?
This requires a payer-specific strategy. While CMS and major national payers have mandated or strongly encouraged the use of X-modifiers since 2015, some smaller or regional payers may not have updated their systems and still require the general Modifier 59. The best practice is to verify each payer's policy. If a payer accepts X-modifiers, using them is essential to demonstrate coding precision. If not, Modifier 59 remains the correct choice. This is where an expert billing partner adds significant value, managing these granular payer-specific rules for fields like anesthesiology billing to ensure compliance and prevent denials.