Vision Medical Billing Services: Maximize Your Revenue 2026
Vision medical billing services are specialized revenue cycle management solutions built to keep ophthalmology and optometry claims on the right payer path, and that matters because up to 30% of annual revenue in optometry clinics is lost to bad debts due to irregular follow-up and claim denials. If your practice is struggling with denials, slow cash flow, or aging A/R, the problem often isn't volume. It's claim routing, split billing, and payer sequencing.
New eye care practices usually assume billing problems start after the visit. In reality, the leak starts before the claim is ever submitted. If your team doesn't separate medical and routine vision workflows at intake, one encounter can trigger a denial, a rebill, staff rework, and delayed cash. We've seen practices focus on exam volume while revenue slips through preventable errors tied to CPT 92014, CPT 92015, modifier 25, and coordination of benefits between medical and vision plans.
What Are Vision Medical Billing Services
Vision medical billing services are specialty RCM services for ophthalmology and optometry practices. Their job is simple to describe and hard to execute well: decide whether each encounter belongs under medical insurance, a vision plan, or both, then build claims that match the documentation, payer rules, and covered services.
General medical billing teams often miss what makes eye care different. Your practice doesn't operate in one claims environment. It operates in two. One side handles disease, injury, and medically necessary diagnostics. The other handles routine eye exams, refraction, and plan-specific vision benefits. If your billing operation treats those as interchangeable, revenue starts leaking fast.
The financial stakes are high. The American Optometric Association highlights that up to 30% of annual revenue in optometry clinics is lost to bad debts due to irregular follow-up and claim denials, and that loss can be reduced with efficient RCM processes, as noted in this discussion of optometry billing challenges and revenue leakage.
What the service actually covers
A strong specialty billing operation usually handles:
- Benefit verification at the right level: Staff must verify both medical and vision eligibility before the visit, not just confirm that the patient is “active.”
- Claim path selection: The claim has to follow the chief complaint and diagnosis, not the easiest payer to bill.
- Split-claim processing: When one visit includes both a medical exam and a refraction, the billing team has to separate them cleanly.
- Denial prevention and follow-up: The work isn't only about posting claims. It's about preventing avoidable rejections and working aging claims before they stall cash flow.
Practical rule: In eye care, your billing team isn't just posting charges. They're making reimbursement decisions that directly affect denial rate, net collections, and A/R speed.
Why practice owners should care
For a practice owner, the value isn't technical elegance. It's fewer denials, faster payment, and less staff time wasted correcting preventable mistakes.
The difference shows up in cash flow. A specialized billing team understands when CPT 92014 supports a medical claim, when CPT 92015 belongs elsewhere, and when a same-day encounter needs separate submission logic. That's what protects margin in a specialty where routine and medical services often happen in the same exam lane.
The Core Challenge Medical vs Vision Plan Billing
The hardest part of eye care billing isn't coding complexity by itself. It's routing each service to the correct payer. Medical and vision claims run on parallel tracks. When a practice sends a claim across the wrong track, the payer doesn't “sort it out.” The payer denies it.
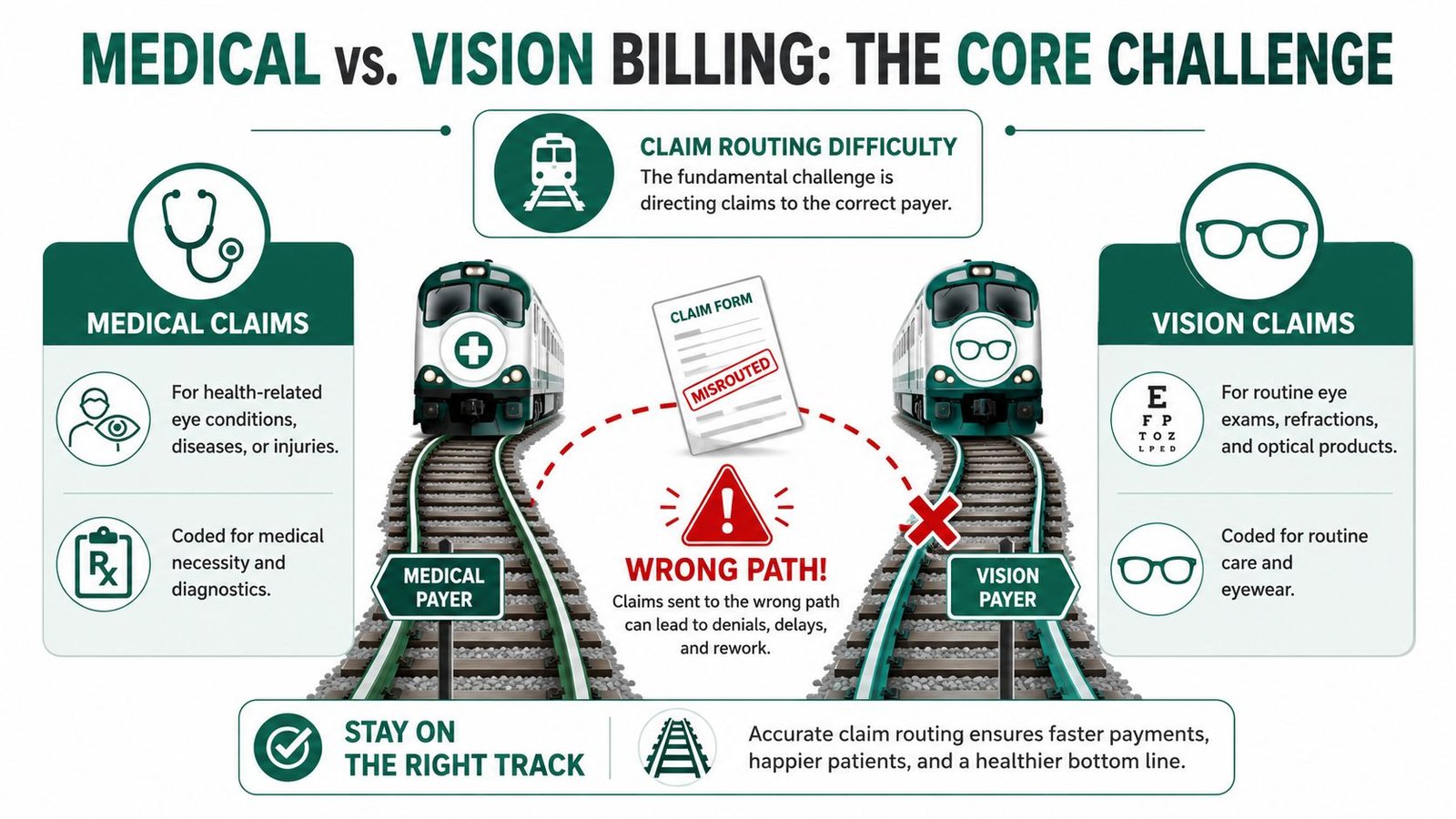
Two payers, two reimbursement models
A disease-related exam billed through medical insurance can reimburse $120–$180, while a routine vision wellness exam may reimburse only $45–$70, according to this overview of medical and vision billing in optometry. The issue isn't only the payment gap. Billing a medical condition to a vision plan, or a routine vision service to medical insurance, leads to automatic denials because the rules are not interchangeable.
Here's the practical split:
| Billing path | Typical use | Common codes | Financial effect |
|---|---|---|---|
| Medical insurance | Disease, injury, symptom-driven exam | 92012, 92014, 99213-99215 with qualifying diagnosis | Higher reimbursement when properly supported |
| Vision plan | Routine exam, refraction, eyewear benefit | 92002, 92004, 92012, 92014, 92015 depending on plan rules | Lower reimbursement, frequency-limited |
That overlap is what confuses non-specialist teams. The same family of eye exam codes can appear in both worlds, but the diagnosis, documentation, and payer rules decide the route.
Where the dual-claim workflow breaks down
The most expensive confusion point is the dual-claim workflow. One patient visit may include a medically necessary eye exam and a refraction. Those are not the same service, and they often should not go to the same payer.
If the patient presents with glaucoma, diabetic retinopathy, dry eye syndrome, or another medical issue, the exam belongs under medical billing. If the same encounter also includes refraction, that portion belongs under the vision plan or patient responsibility depending on coverage. Practices that try to force everything through one payer create denials, rebills, and staff churn.
A denial in this setting usually means your staff has to touch the same encounter again at least once. Sometimes several times. That's expensive even before you count the delayed cash.
The vendor question is whether your billing partner can automate that split without relying on manual memory. The right system should read chief complaint, verify both coverages, flag CPT 92015 separately, and stop staff from bundling unrelated services into one claim. That's the difference between scalable billing infrastructure and a front desk workaround.
For owners reviewing coding support, the broader question of component billing also matters, especially in imaging-heavy specialties. This resource on modifier 26 vs TC is useful when evaluating whether a billing vendor understands professional and technical charge separation.
Common Revenue Leaks in Ophthalmology and Optometry
Most revenue loss in eye care doesn't come from one catastrophic mistake. It comes from a stack of small billing errors that repeat every day. One claim is missing the right modifier. Another includes a diagnostic test without strong medical necessity support. Another sits in pending status because staff billed the wrong payer first.

The modifier 25 leak
One of the most common examples is modifier 25. In our audits of over 120 optometry practices, 38% of denied claims for eye exams (CPT 92014) were due to a missing modifier 25, contributing to an average annual revenue loss of $28,000 per practice, tied to AAPC guidance on the relevant CPT code range.
If your physician performs a separately identifiable exam on the same day as another billable service and the modifier isn't applied correctly, the payer may bundle the services and deny reimbursement for the exam portion. Practice owners often see this as a coding detail. It isn't. It's a direct revenue problem.
Imaging and documentation failures
Another common leak happens with diagnostic imaging. Codes like 92250 for fundus photography and 92133 for optic disc scans need medical necessity documentation that matches the service. If the note doesn't support why the test was performed, the claim may be rejected or written off.
That creates two losses at once:
- Lost reimbursement for the test itself
- Staff time spent appealing a claim that should have been clean on first submission
Clean documentation is a billing asset. In ophthalmology and optometry, diagnostic testing without tight documentation turns a clinical service into an administrative expense.
Manual denial work compounds quickly
Practices also lose money when they normalize manual correction. The front desk knows one payer likes the claim one way. The biller knows another payer wants separate sequencing. Someone keeps a spreadsheet. Someone else remembers to override the system. That works until volume rises, turnover hits, or a physician adds another location.
That's usually when denial patterns become visible. If you're investigating those patterns, this guide to medical billing denial management is a useful framework for identifying whether the issue is coding, eligibility, documentation, or payer sequencing.
The takeaway is simple. Revenue leaks in eye care are usually operational, repetitive, and fixable. The danger is that they don't look urgent until they've already widened your A/R.
The Financial Case for Outsourcing Your Vision Billing
Outsourcing vision medical billing services makes sense when your internal team is spending too much time correcting preventable errors instead of collecting cash. The financial benefit isn't theoretical. It shows up in fewer touches per claim, cleaner submissions, and faster payment cycles.
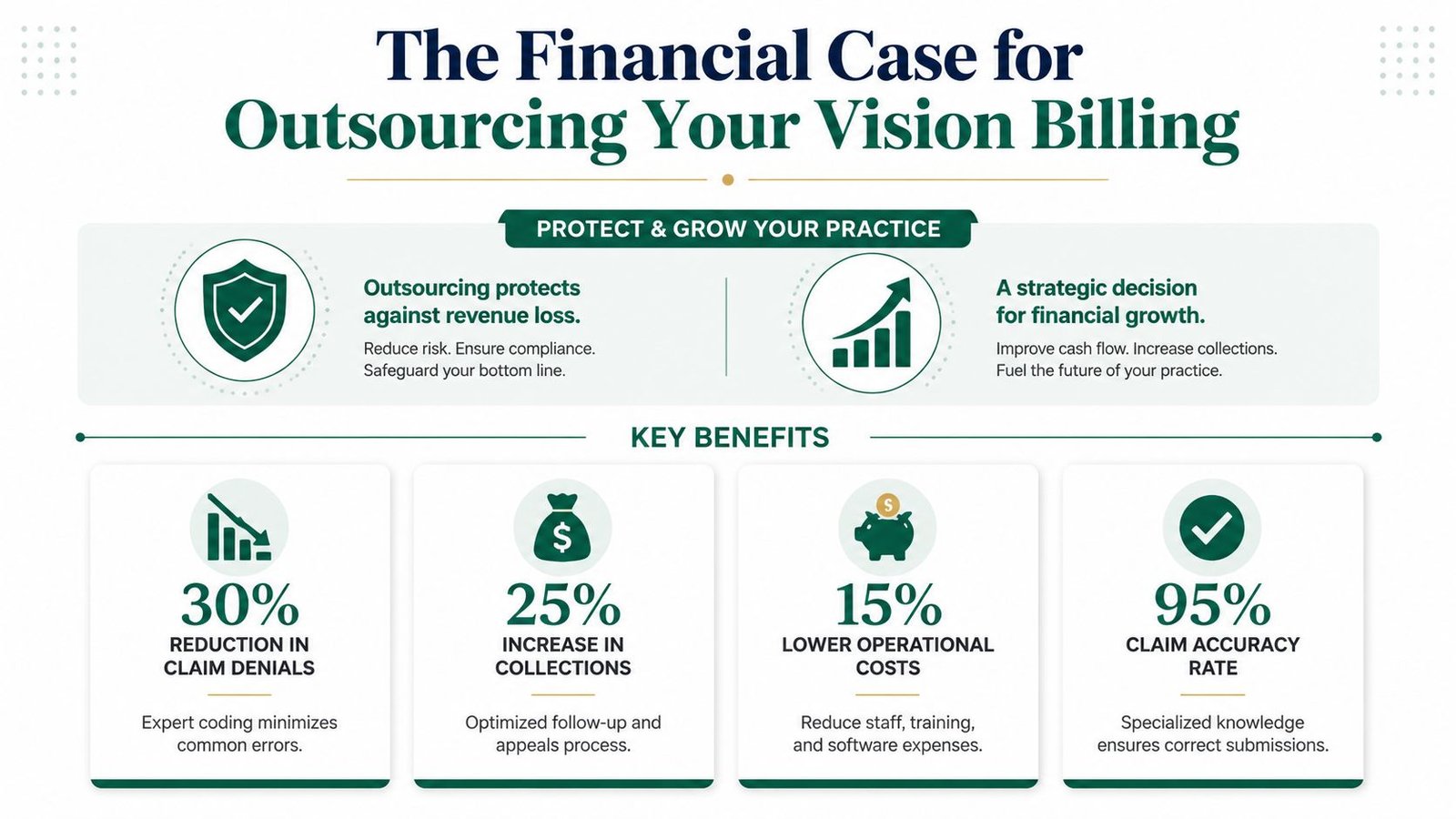
What strong specialty outsourcing changes
Practices that use AI-driven billing platforms with expert human oversight consistently achieve days in A/R under 35 and first-pass clean claim rates exceeding 98%, compared to traditional methods averaging 45–50 days in A/R and 85–90% clean claims, based on this analysis of ophthalmology medical billing services and performance benchmarks.
That gap matters for an owner because every day added to A/R slows hiring, vendor payments, equipment purchases, and physician distributions. Cleaner claims also reduce the hidden labor cost of rework.
The hidden cost of keeping billing in-house
The internal argument for keeping billing in-house is usually control. In practice, many groups keep the workload, the turnover risk, and the training burden, while losing control of outcomes.
A specialized billing partner should already know how to handle:
- Dual-claim workflows: Medical exam to the medical payer, refraction handled separately
- Payer-specific edits: Different rules for Medicare, Medicaid, commercial plans, VSP, or EyeMed
- Denial prevention logic: Catching modifier errors, sequencing problems, and eligibility conflicts before submission
- Operational continuity: Claims still move when a front-office employee quits or takes leave
If staffing is part of your broader operations challenge, it helps to look at adjacent healthcare workflows too. This expert guide for healthcare HR is useful because billing performance often falls apart when practices can't hire or retain the right operational support fast enough.
Outsourcing should improve economics, not just convenience
The right decision isn't “outsource because billing is annoying.” It's outsource when a specialist can protect more revenue than your current setup can reliably collect.
A practical way to evaluate that is to compare your current staffing, software, denial follow-up, and leadership oversight costs against a specialist model. This resource on what outsourced medical billing costs is helpful when you're deciding whether your current process is cheaper, or just less visible.
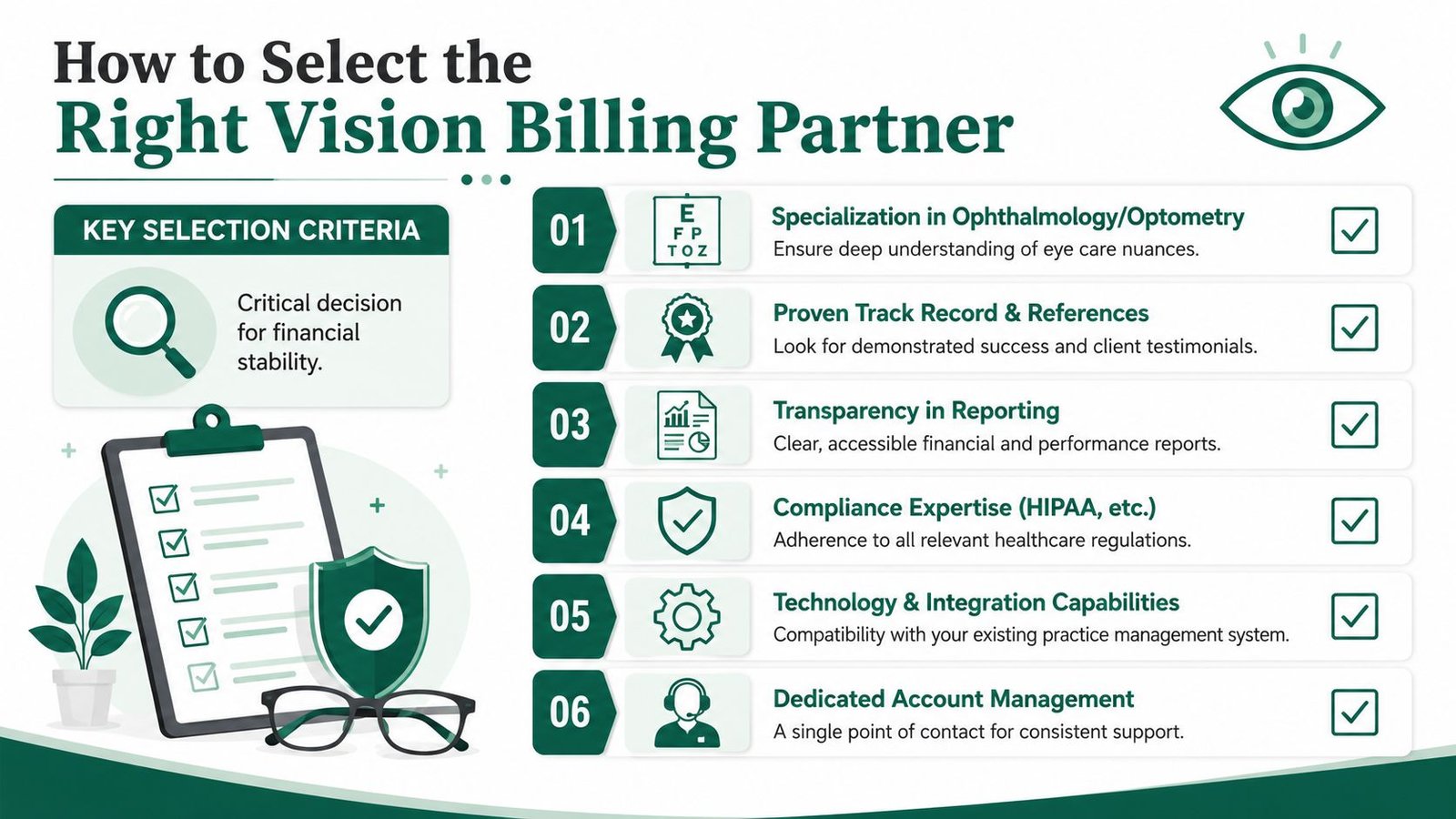
How to Select the Right Vision Billing Partner
Most billing vendors can say they handle ophthalmology or optometry. Far fewer can manage the details that effectively protect revenue. The wrong partner will submit claims and send reports. The right partner will stop preventable denials before they happen, especially in split-claim encounters where medical and vision coverage overlap.
Start with coordination of benefits capability
In our experience, improper coordination of benefits between medical and vision plans causes a 15–22% increase in denial rates, and practices that outsource COB management reduce their denial rate by an average of 34% and cut days in A/R from 52 to 31 within six months, as described on this specialty billing overview for complex practices.
That one area tells you a lot about a vendor. If they can't explain who gets billed first when a patient has both medical and vision coverage, they aren't ready for your practice.
Ask direct questions:
- How do you sequence primary and secondary claims when one visit includes a medical exam and a refraction?
- How do you prevent duplicate billing flags?
- How do you document payer-specific rules inside the workflow so staff doesn't rely on memory?
Look for operational traits, not marketing language
A strong partner should be able to answer these without hesitation:
| What to evaluate | Why it matters to the owner |
|---|---|
| EHR integration | You don't want a disruptive migration just to fix billing |
| Specialty coding depth | Eye care billing requires more than generic claim submission |
| Real-time reporting | You need visibility into denials, A/R, and payer trends |
| HIPAA-first controls | Billing access touches PHI, payment data, and audit risk |
| Human review layer | Automation catches speed issues, auditors catch nuance |
Demand proof in workflow terms
We've found that the best screening question is not “How many clients do you have?” It's “Show me how you handle a same-day medical exam plus refraction with dual coverage.”
If the vendor answers with generalities instead of a defined workflow, they'll probably discover your denials at the same time you do.
You should also ask how they measure performance after go-live, what dashboard access you'll receive, and who owns appeals for payer-specific denials. This checklist of questions to ask a medical billing company before hiring is a practical starting point for that discussion.
Measuring Success KPIs and ROI Scenarios
A small drop in collection performance can erase more profit than most new practice owners expect. In eye care, the losses usually show up in rework, delayed cash, and dual-claim errors that never get corrected.
That is why billing KPIs need to measure cash movement, not just claim volume. A claim submitted to the wrong payer still counts as “worked” in many dashboards. It does not count as revenue.
The KPIs that matter in eye care
Start with four numbers:
- First-pass clean claim rate: How often claims pay without edits, rebills, or added documentation
- Days in A/R: How long it takes to turn charges into collected cash
- Denial rate: How often your team is creating preventable payer problems
- Net collection rate: How much of your allowed revenue you collect
For a structured benchmark, review these medical billing KPIs to track. The right scorecard should break performance down by payer, provider, location, and denial category.
A general RCM dashboard is not enough for ophthalmology or optometry. You also need visibility into the dual-claim workflow. How many encounters involved both a medical plan and a vision plan? How many required manual correction before submission? How many sat in hold status because staff could not determine payer order, refraction handling, or patient responsibility? If your vendor cannot report on those points, they are hiding labor inside the process.
The same rule applies in other operational systems. Teams that study how to track chatbot performance already know that activity metrics mean very little unless they tie to the business result. Billing works the same way. Posted payments, reduced rework, and faster cash matter. Raw claim counts do not.
ROI starts with the dual-claim failure rate
The clearest ROI model in vision medical billing is often the simplest one. Measure how much staff time and collectible revenue you lose when a same-day medical exam plus refraction is handled manually.
Here is where owners usually bleed margin:
- The medical claim goes out first, but the vision portion never gets billed
- The refraction is attached to the wrong payer and has to be reversed or written off
- Staff hold mixed encounters for manual review, which slows cash and grows A/R
- Front-desk estimates are wrong, so patient balances age instead of collecting at check-out
Those problems do not look dramatic one claim at a time. Across a month, they create extra touches on the same encounter, slower secondary billing, and more small balances that cost more to chase than they are worth.
A capable billing partner should be able to show you the before-and-after impact in operational terms: fewer touches per dual-coverage encounter, shorter time from date of service to final payment, lower denial volume tied to coordination errors, and higher point-of-service collection accuracy.
What good performance review looks like
A monthly review should answer a few direct questions:
- Which denials were preventable at registration or charge entry?
- How many dual-claim encounters required manual intervention?
- Which payer combinations create the most rework?
- Which providers or locations have the highest rate of underbilling, write-offs, or delayed secondary submission?
- How much staff time is being spent correcting vision-versus-medical routing mistakes?
If your billing partner cannot answer those questions with current reporting, you are not managing eye-care revenue well enough. You are reacting to it.
For one payer-specific example, Medicare states that refractions are not covered, including CPT 92015, in its patient guidance on routine eye exams and refractions at Medicare coverage for eye exams and refractions. If your workflow sends those charges to Medicare by default, staff will spend time fixing avoidable errors, and some of that revenue will never be recovered.
Good ROI reporting is not complicated. It should show whether your billing operation is reducing manual work, protecting collectible services, and closing the gap between what you performed and what you deposited.
Frequently Asked Questions from Practice Owners
Can my EHR's built-in billing module handle vision billing on its own
Usually not. Built-in billing modules can submit claims, but dual-claim eye-care billing depends on rule logic that many standard setups do not manage well. The primary difficulty is splitting the encounter correctly between medical and vision coverage, then sequencing both claims without creating duplicate work, filing delays, or coordination errors.
I see practices lose money here in two ways. Staff send the whole visit to the wrong payer, or they correct it manually after the first denial. Both outcomes slow cash and raise labor cost on encounters that should have been routine.
Is outsourcing still worth it for a smaller independent practice
Yes, if your team is spending too much time fixing preventable billing mistakes. Smaller practices usually feel dual-claim errors faster because one missed secondary submission or one unresolved vision-plan edit can affect weekly cash flow, not just month-end reporting.
The question is not your practice size. The question is whether your current process handles co-billing accurately enough to protect revenue without pulling your front office into back-end rework.
How disruptive is the transition to a new billing partner
A good transition is controlled and specific. The billing partner should review payer setup, map medical and vision plan rules, test dual-claim workflows, clean up open A/R, and identify where staff are using manual workarounds that create rework later.
Avoid vendors that speak in general medical billing terms but cannot explain how they post, route, and reconcile same-day medical and vision encounters. In eye care, that gap shows up quickly in denials, aging, and under-collected patient balances.
What should I ask before signing with a vision billing company
Ask direct questions:
- How do you split and sequence dual claims for the same date of service?
- Which payer combinations still require manual intervention in your workflow?
- How do you prevent modifier 25 misuse and diagnosis mismatches?
- Who owns coordination of benefits and secondary follow-up?
- Can you show reporting on dual-claim touch rate, denial causes, and days to final payment?
- How do you reduce staff workarounds inside our current EHR and PM system?
If the answers are vague, the process is probably manual behind the scenes. That means higher hidden labor cost for your team and more missed revenue than your monthly collections report shows.
If your ophthalmology or optometry practice is writing off avoidable denials, chasing secondary claims too late, or relying on staff to manually patch medical versus vision billing decisions, Happy Billing can help you identify the exact failure points. Their team works inside existing systems, understands eye-care-specific payer logic, and can review your workflow to show where dual-claim errors, posting gaps, and manual workarounds are draining margin.