Expert Medical Billing Services Dallas: Boost Your Revenue

Monday morning in a Dallas practice often starts the same way. The schedule is full, the physicians are working, and the bank balance still does not reflect the volume because claims are stalled by eligibility errors, authorization gaps, and payer-specific edits that should have been caught before submission.
If you're evaluating medical billing services in Dallas, judge the vendor by what happens to cash in the next 30 to 60 days. A good partner improves first-pass acceptance, shortens A/R cycles, and finds leakage at the front desk, in coding, and in follow-up before it turns into write-offs. For many groups, the best fit is a team with real experience in Texas medical billing services for multi-payer practices, not a generic national shop applying the same workflow to every market.
Dallas adds a layer many billing companies underplay. Texas Medicaid MCO rules vary by plan, prior authorization requirements shift, and a practice that serves Spanish-speaking patients loses money fast if billing staff cannot explain balances, obtain missing insurance details, or resolve follow-up questions without friction. I have seen otherwise solid practices collect less because patient statements, call handling, and payment conversations were not built for a bilingual market.
Revenue leakage rarely starts with one major breakdown. It usually starts with small misses that stack up. Eligibility is not verified correctly. An authorization does not match the rendering provider or service date. E/M coding trends conservative and leaves money on the table. Denied claims age past timely filing. Vendor selection matters here, and practices that apply effective vendor management strategies tend to spot these problems earlier and hold billing partners to measurable standards.
The goal is straightforward. Get claims out clean, get paid faster, and stop preventable denials before they become a monthly pattern.
Choosing the Right Dallas Medical Billing Service
A strong Dallas billing service isn't the one with the nicest dashboard. It's the one that protects your revenue when the front desk is busy, your physicians are overbooked, and payers are looking for reasons to reject claims.
Many practice owners are in the same spot. Care delivery is solid, volume is steady, but cash flow feels uneven. Your team works claims after hours, A/R creeps up, and every month ends with the same question: why are collections lagging when the schedule was full?
What good looks like in Dallas
The standard should be practical and measurable. In Dallas, the better-performing practices don't just submit claims quickly. They submit claims that pay the first time, and they don't let unresolved A/R age into a habit.
Structured outsourced RCM in major markets like Dallas can produce a 30 to 40% reduction in claim denial rates within two billing quarters, largely through better eligibility verification and prior authorization management (denial reduction data). That's the difference between a billing vendor and an actual revenue partner.
A billing company should lower your rework load, not simply take over it.
For many physicians, the wrong comparison is “outsource versus keep billing in-house.” A more accurate comparison is “predictable collections versus recurring leakage.” If your current process misses modifier opportunities like -25 on separately identifiable E/M services or mishandles global-period billing in surgical specialties, the financial loss doesn't show up as one line item. It shows up as slower deposits, more write-offs, and higher administrative drag.
What to ask before you sign
A Dallas practice should judge vendors on operating discipline, not sales language. Look for:
- Front-end control: Can they verify eligibility at scheduling and again at check-in?
- Authorization rigor: Can they show a repeatable workflow for prior auth, especially for Texas plans?
- Specialty fluency: Do they understand the codes and modifiers that generate your revenue?
- Reporting clarity: Can they show you NCR, denial categories, and aged A/R in a way a physician can act on?
If you're comparing multiple firms, it helps to apply the same procurement discipline you'd use with any strategic service partner. These effective vendor management strategies are useful because they force accountability around reporting, scope, and service levels. For a Texas-focused overview of what outsourced support should include, review medical billing services in Texas.
The Core Metrics That Define Billing Success in Texas
Monday morning in a Dallas practice usually tells you more about billing performance than any sales deck. The schedule is full, Friday's charges are still trickling in, two Texas Medicaid MCO claims are stuck for authorization-related reasons, and your front desk is trying to explain a patient balance in English to a Spanish-speaking family who never understood the statement. Those are not separate problems. They show up in the same places: denials, delayed cash, and collectible dollars that never reach the bank.
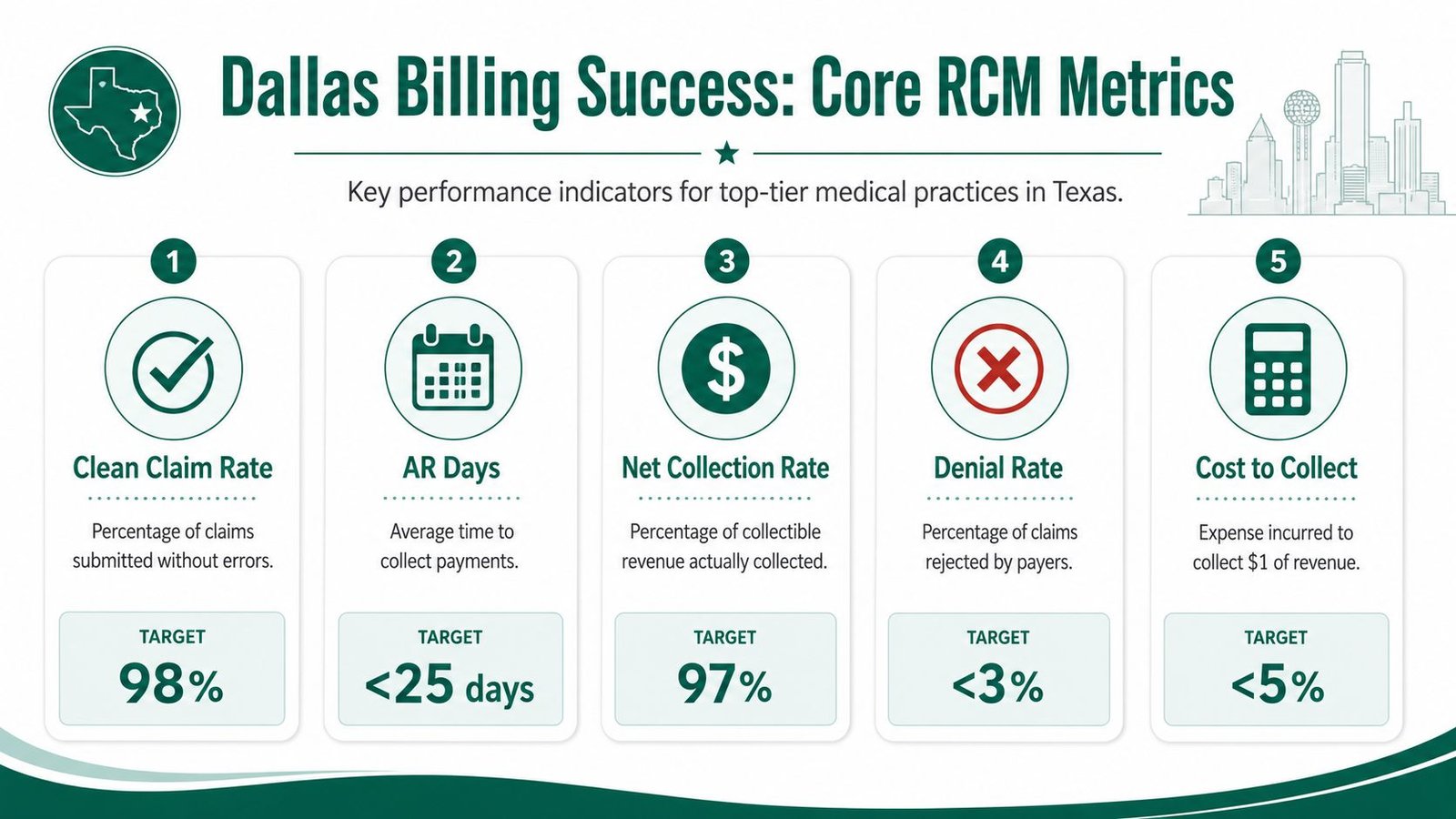
First-pass clean claim rate
First-pass clean claim rate measures whether your process catches errors before the payer does. In Texas, that means more than checking demographics and eligibility. It includes payer-specific authorization rules, correct Medicaid MCO routing, referral status, modifier use, and documentation that supports the code set submitted.
A clean claim problem is rarely a billing-office-only issue. It usually starts at scheduling, registration, or charge entry. One missed referral, one invalid member ID, or one poorly supported modifier can turn a claim that should have paid in the next cycle into a denial that sits 30 to 45 days before anyone touches it again.
Texas practices should also watch this metric by payer, not only in aggregate. A vendor can post a respectable overall clean claim rate while repeatedly failing with a few high-volume plans. That is common with Medicaid managed care and with payers that enforce prior authorization edits aggressively.
Days in A/R
Days in A/R shows how long your revenue cycle is financing operations. Once this number rises, the practice feels it fast. Payroll pressure increases, physician compensation gets tighter, and staff time shifts from prevention to rework.
In Dallas, I pay close attention to A/R by financial class and by aging bucket. Commercial claims aging out is one problem. Medicaid MCO balances over 90 days are another. They often require a different escalation path, different documentation, and tighter appeal discipline. If your billing partner reports one blended A/R number without separating those categories, you cannot see where cash is getting stuck.
Patient A/R matters too. Practices that lack bilingual phone support and bilingual statements collect more slowly from Spanish-speaking households. That is not a soft service issue. It is a cash-flow issue. If the patient does not understand the balance, payment timing slips, call volume rises, and balances roll into bad debt. For office managers handling statements and self-pay follow-up, understanding the dunning process helps connect patient communication to recovery rates after insurance adjudication.
Net collection rate
Net collection rate is the clearest test of whether your billing partner protects collectible revenue after contractual adjustments. If this number is weak, the practice is losing money somewhere. Usually the causes are avoidable write-offs, underpayments that go unworked, filing deadline misses, or denials that should have been prevented upstream.
Low vendor pricing stops mattering; a cheaper billing service that misses underpayments or lets timely filing deadlines pass costs more than a higher-fee partner with disciplined follow-up and payer-specific controls.
For Texas groups, I also want net collection rate broken down by payer and provider. That exposes patterns a summary report hides. If one provider has stronger denial rates tied to documentation, fix the documentation. If one payer consistently pays below contract, audit the remits and escalate. If Texas Medicaid MCO claims have lower net collections than expected, review authorizations, eligibility checks, and appeal turnaround first.
A useful monthly scorecard should include:
- Clean claim rate by payer: to catch front-end failures before denials stack up
- Days in A/R by aging bucket and financial class: to show where cash is slowing down
- Net collection rate by payer and provider: to spot underpayments and preventable write-offs
- Denial categories with volume and dollars: to identify the exact sources of leakage
- Patient collection performance: to measure whether statement timing, call workflows, and language access are helping or hurting recovery
If you want a practical template your team can review every month, this guide on medical billing KPIs to track is a useful starting point.
Non-Negotiable Capabilities for Your Billing Partner
A vendor can sound competent in a sales call and still create operational drag once claims start flowing. In our experience, the right billing partner is defined less by marketing language and more by a short list of capabilities that directly protect collections.
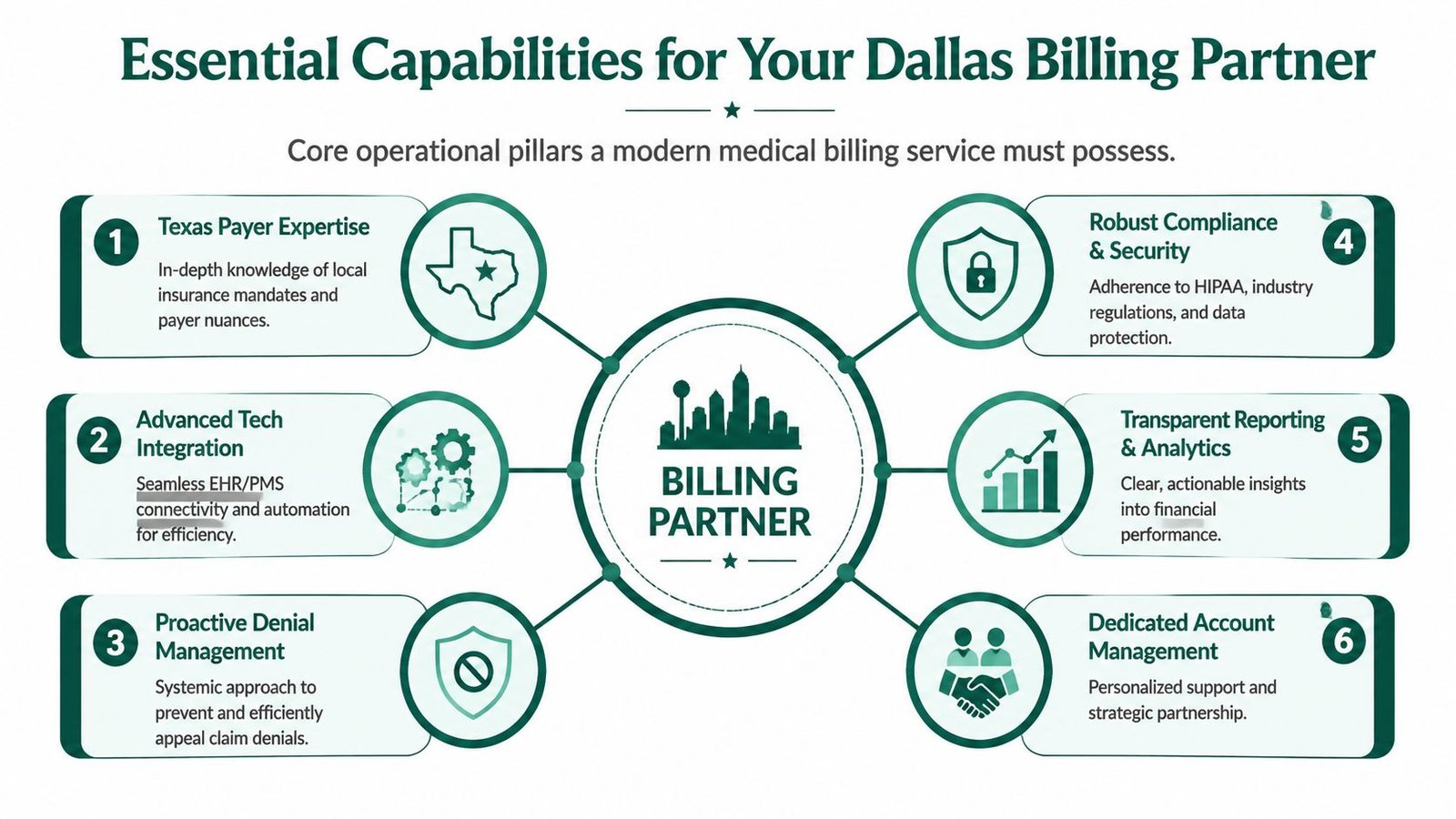
EHR and practice management integration
A billing company should work inside your current environment whenever possible. Forced migration creates disruption, weakens accountability during transition, and usually introduces new errors before old ones are solved.
We've seen practices lose momentum when a billing vendor wants to replace systems instead of mastering the existing workflow. If your physicians document in one system and billing wants another, the handoff points multiply. That's where missing charges, lagging notes, and documentation-to-claim mismatches start.
For procedure-heavy specialties, this has a direct cash effect. Orthopedic claims billed during global periods, anesthesia claims tied to time units and concurrency, and cardiology claims involving procedural edits all depend on clean documentation flow from the original chart.
Texas payer expertise
National billing firms often underperform in Dallas because they treat Texas payers as interchangeable. They aren't. Texas Medicaid MCO workflows, local plan quirks, and authorization rules require more than generic payer knowledge.
That's especially true when claims depend on strict payer sequencing and coverage confirmation before submission. CMS rules, payer bulletins, and AAPC coding standards all matter, but the daily revenue impact comes from whether the billing team can operationalize them. If they can't, your physicians end up writing off avoidable denials that began at intake.
Denial prevention before denial management
Most vendors talk about denial management. Fewer can explain how they reduce denials before a claim leaves the system.
The essentials include:
- Eligibility checks at two points: Scheduling and check-in
- Authorization matching: Procedure, diagnosis, date range, and payer-specific requirements must align
- Claim scrubbing: Edits for demographics, coding, and modifier logic before submission
- Documentation review: Especially for E/M services, procedures with bundling risk, and claims requiring medical necessity support
If your practice bills common office visit codes like 99213 or 99214, or transitional care codes such as 99495, the risk isn't just coding accuracy. It's whether documentation, timing, and payer rules support the billed service in a way that survives review. For a plain-language explanation of one high-value code family, this overview on improve patient outcomes with CPT 99495 is helpful background, especially when evaluating whether a vendor understands post-discharge revenue opportunities.
The best denial strategy starts before the patient arrives, not after the ERA posts.
Compliance, security, and reporting
HIPAA compliance should be assumed. What matters is whether the vendor can explain how access is limited, how PHI is handled, and how activity is monitored. If the answer is vague, move on.
Reporting matters just as much. A physician owner should be able to review monthly performance without decoding a spreadsheet. At minimum, you should see payer-specific denials, aged A/R, collections trend, unresolved authorization issues, and reason-code patterns that point to process fixes.
Specialty depth
Generalist billing sounds efficient until specialty complexity appears. An anesthesiology group needs accurate handling of modifiers and concurrency logic. An orthopedic group needs disciplined treatment of postoperative global rules and multiple-procedure issues. A behavioral health group needs authorization-centric billing that prevents mismatch denials before claim submission.
If you're comparing firms, this checklist for choosing the best medical billing company is useful because it pushes beyond generic promises and into operational proof.
Decoding Billing Service Costs and Contracts
Most practices focus first on the vendor's percentage. That's understandable, but it's rarely the smartest starting point. The better question is whether the cost model aligns with your volume, specialty complexity, and tolerance for fixed overhead.
Independent practices in Dallas that hire a dedicated RCM specialist face annual labor costs of $48,000 to $52,000 before benefits (Dallas RCM salary data). Once you add management time, coverage gaps, training, and turnover risk, in-house billing becomes a heavier fixed expense than many owners expect.
Medical Billing Service Cost Models Compared
| Model | How It Works | Best For | Key Consideration |
|---|---|---|---|
| Percentage of collections | Vendor takes a percentage of collected revenue | Practices that want aligned incentives and variable cost structure | You need clear definitions of what counts as collections and who owns old A/R |
| Flat fee per claim | Vendor charges per claim submitted or processed | High-volume, predictable claim environments | Cheap per-claim pricing can become expensive if denial follow-up is excluded |
| Fixed monthly fee | Practice pays a set monthly amount | Stable practices with consistent volume and narrow scope | Works best when contract language clearly defines included services |
The hidden cost isn't always the invoice
A low monthly fee can look attractive until the exclusions surface. We often see contracts that separate core revenue functions into chargeable add-ons. Denial appeals, prior authorization support, patient statements, credentialing, and legacy A/R recovery may not be included in the base price.
That matters because these aren't optional side tasks. They're where revenue is either protected or lost. If your group bills time-sensitive post-discharge services, procedure-heavy encounters, or frequent E/M claims, weak follow-through can erase any apparent savings.
Contract terms that deserve scrutiny
Before you sign, review the agreement for these issues:
- Term length: Long lock-ins protect the vendor, not your practice
- Data ownership: Your reports, payer credentials, and claim history should remain fully accessible
- Scope definition: Clarify whether coding review, denial appeals, patient statements, and old A/R are included
- Performance visibility: If the contract doesn't require regular reporting, expect ambiguity later
Cheap billing fees often mask expensive revenue leakage.
Another trap is judging cost without considering net collections. A percentage-based fee can be the better financial choice if the vendor reduces leakage and accelerates payment. A flat-fee vendor can be the more expensive option if your staff still has to resolve denials, answer payer questions, and clean up submissions internally.
If you're trying to compare these models in a more structured way, this guide on outsource medical billing cost gives a useful framework for evaluating what you're really paying for.
The Vendor Interview Your Practice Must Conduct
Monday morning in a Dallas practice often starts the same way. A full schedule is on the books, a few patients arrive with coverage issues, one procedure needs an authorization check, and last week's denied claims are still sitting in aging. If your billing vendor cannot explain exactly how they prevent those failures before the claim drops, the interview is not doing its job.
A useful vendor interview tests operating discipline under Texas conditions. Dallas groups need more than a polished overview of software and reports. They need to know how the billing team handles Texas Medicaid MCO rules, payer-specific edits, front-desk handoffs, and Spanish-language patient communication that affects collections and claim accuracy.

Questions that reveal whether the vendor is real
Ask questions that force the vendor to describe workflow, ownership, and escalation. Vague answers usually mean your staff will end up doing cleanup work later.
- How do you verify eligibility and benefits before the visit? Look for a two-step process tied to scheduling and check-in, with a clear plan for documenting copays, deductibles, and coverage limits before service.
- How do you prevent authorization-related denials? The right answer should include matching CPT, diagnosis, payer requirements, rendering provider, and date span before claim submission.
- How do you handle modifier-sensitive claims? Ask for specialty-relevant examples using -25, -59, -24, or other modifiers your group depends on to protect reimbursement.
- What happens after a denial posts? Serious vendors sort denials by category, assign follow-up responsibility, track appeal deadlines, and report root causes so the same issue does not keep draining revenue.
- How do you support Spanish-speaking patients? Ask whether bilingual outreach is part of the service, who handles patient balance questions, and how language support affects intake accuracy and payment follow-up.
Texas-specific questions that generic scorecards miss
Texas payer complexity changes the interview. If the vendor works Dallas A/R every day, they should be able to speak plainly about Texas Medicaid managed care plans, authorization status checks, and the documentation gaps that trigger rejections.
For behavioral health, ask how they confirm Texas Medicaid MCO authorizations before claims go out and what they do when the approved service does not match the scheduled service. For orthopedic groups, ask how they protect revenue during global periods and how they document separately billable work without creating modifier risk. For anesthesiology, ask how they audit time units, concurrency, and medical direction support before filing. For cardiology, ask how they resolve payer edits around diagnostic versus interventional services.
The point is simple. If a vendor cannot connect a workflow failure to delayed cash and avoidable write-offs, they have not managed enough at-risk revenue in your specialty.
What strong answers sound like
Good answers are specific. The vendor should be able to describe who reviews eligibility, who checks authorization details, what claim edits run before submission, how often denials are reviewed, and which reports your practice sees each month. I also want to hear target ranges. A vendor that manages performance seriously should be comfortable discussing first-pass acceptance rate, denial rate, days in A/R, and the time to rework denials.
Weak answers stay broad. “We handle everything” usually means the process lives in someone's head, not in a repeatable workflow.
Use a written scorecard during every interview. Grade each vendor on specialty fit, Texas payer knowledge, bilingual support, denial prevention, and reporting clarity. This checklist of questions to ask a medical billing company before hiring gives you a practical structure for comparing vendors side by side.
Onboarding and Transition A Painless Checklist
Switching billing partners doesn't have to disrupt patient care or cash flow. Problems usually happen when the transition is vague, rushed, or treated as a software event instead of an operational handoff.
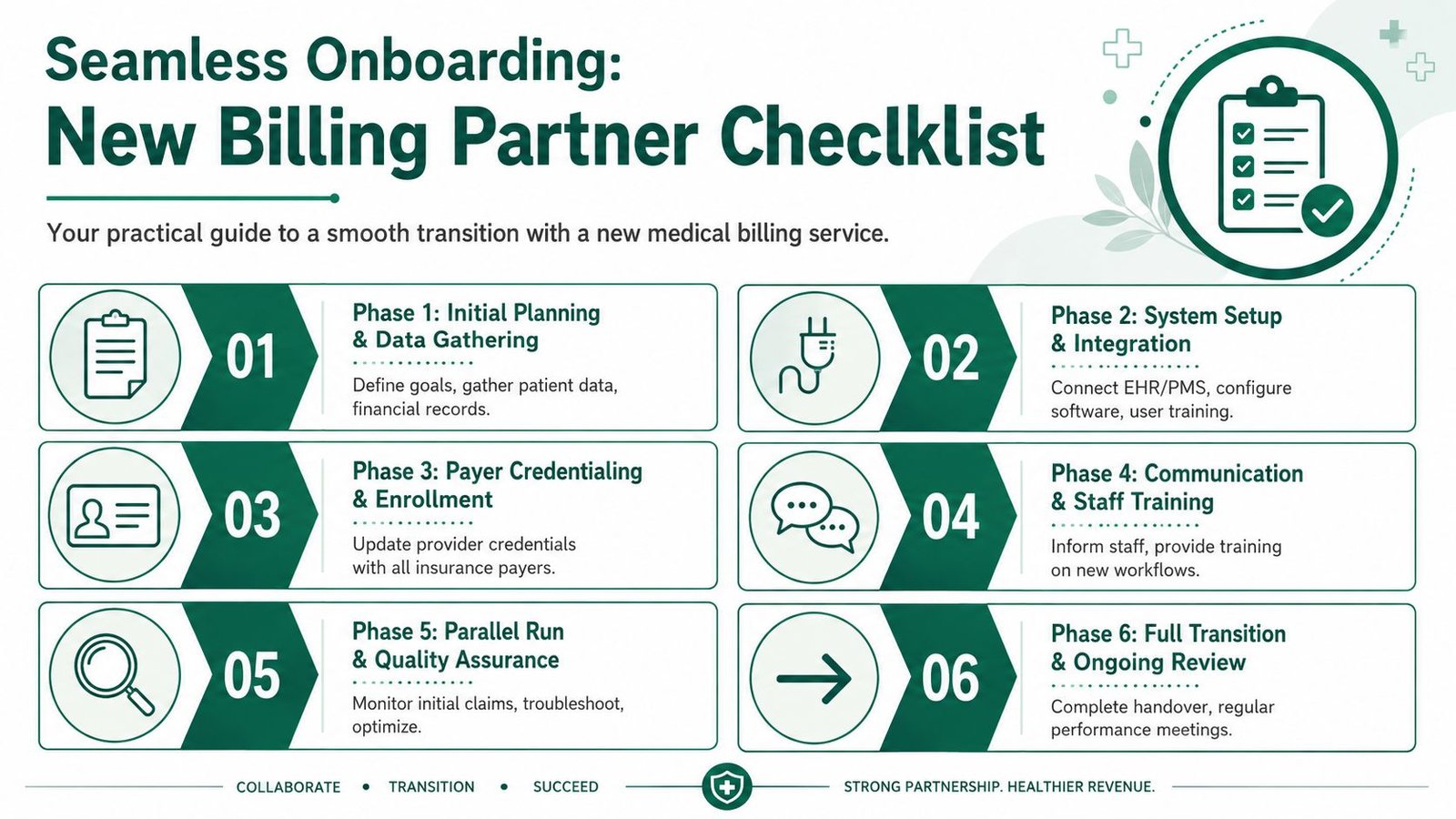
Phase one through phase three
The first step is a practical kickoff. Define which payers, providers, locations, and service lines are in scope. Confirm who owns credentialing follow-up, old A/R, patient statements, and unresolved denials.
Then lock down system access. The cleaner model is for the billing partner to work inside your existing EHR and practice management system so documentation, charges, and payments stay visible in one place. During this stage, payer enrollments and provider rosters should also be verified.
For behavioral health practices, transition discipline matters most. Texas Medicaid rejections for mental health claims average 18% higher than commercial claims due to authorization mismatches, and fewer than 5% of Dallas billing vendors explicitly address Texas-specific authorization-centric workflows for mental health (Texas mental health billing data). If your onboarding plan doesn't include authorization status checks before submission, you are carrying known revenue risk into the new relationship.
Phase four through phase six
Once access and payer setup are stable, train the staff who affect revenue upstream. Front-desk teams need to know exactly what must be captured at scheduling and check-in. Clinical staff need clarity on documentation timing, missing elements, and charge entry expectations.
A good transition also includes a short parallel review period. That means watching initial claims closely, verifying ERA posting logic, and checking whether edits are being resolved where they originate. Early reporting should focus less on glossy dashboards and more on whether claims are moving cleanly.
Use this checklist during onboarding:
- Confirm provider enrollment: Make sure every active payer profile is current before claims flow
- Define communication lanes: Decide who handles urgent denials, payer escalations, and documentation questions
- Set reporting cadence: Weekly early reviews work better than waiting for a month-end surprise
- Match workflows to specialty: Orthopedics, for example, needs close attention to global periods and postoperative billing boundaries
If your group spans multiple service lines, it helps to review how billing workflows differ by specialty. The pages under specialty-specific billing support are useful for seeing how onboarding should be adapted, including for orthopedic practices navigating global periods.
Frequently Asked Questions
How quickly can we see an improvement in collections after switching?
In our experience, the first gains usually come from front-end cleanup. When eligibility checks, authorization review, and claim edits are tightened early, denial pressure often drops first, and collections follow. The biggest mistake is expecting old A/R cleanup alone to fix cash flow if current claims are still being submitted with preventable defects.
My practice is a niche specialty. How do I know a billing service truly understands my coding?
Ask them to explain the codes, modifiers, and payer rules that drive revenue in your specialty. An anesthesiology vendor should be comfortable discussing time units, concurrency, and relevant modifiers. An orthopedic billing team should understand global periods and when separate E/M billing is appropriate. A real specialist speaks in operational terms, not broad promises.
What's the biggest mistake practices make when choosing a billing service in Dallas?
They focus too much on the fee and not enough on collection performance. A cheaper contract doesn't help if denials stay high, A/R stretches, and collectible revenue is missed. The better decision is the one that protects revenue after the invoice is paid.
Should we outsource billing or fix our current in-house team?
That depends on whether the problem is staffing or system design. If your team is capable but unsupported, stronger workflows and accountability may solve it. If the practice is carrying repeated denials, uneven follow-up, weak reporting, and high fixed labor burden, outsourcing can turn billing from a staffing problem into a disciplined revenue function.
Happy Billing helps physician groups tighten revenue cycle performance without forcing EHR migration, combining AI-assisted workflows with expert human review to reduce denials and accelerate cash flow. If your practice wants a clear view of where money is leaking, start with a free billing audit from Happy Billing or explore Happy Billing to see how specialty-focused RCM support works in practice.