No Surprises Act Compliance: A Guide for Practice Owners
No Surprises Act compliance is not optional if you want predictable cash flow. It requires patient communication workflows, Good Faith Estimates for uninsured or self-pay patients, and dispute handling discipline, because when those controls break, revenue gets tied up in rework, write-offs, and avoidable A/R drag.
If you're running a physician practice, this usually shows up first as an operations problem, not a legal one. A patient questions a bill. Your front desk says one thing, billing says another, and the payer has already pushed the claim into delay or dispute. That is revenue sitting still. It also burns staff time you should be spending on scheduling, collections, and denial prevention.
Why No Surprises Act Compliance Is a Revenue Issue
A lot of owners still treat the No Surprises Act as a compliance memo. That's a mistake. It belongs inside revenue cycle management.

The law took effect on January 1, 2022, and CMS later reported that as of June 30, 2024, it had received more than 16,000 complaints, closed 12,700, identified 400 complaints with PHS violations, and reported $4.3 million in fines and other enforcement actions by that date, according to this compliance summary of CMS enforcement activity. If you're a practice owner, those numbers tell you one thing. This is being enforced, and sloppiness is expensive.
Where practices lose money first
Most practices don't feel the pain as a federal headline. They feel it in smaller, uglier ways:
- Delayed collections: Staff holds statements or rebills accounts because nobody is sure whether a patient can legally be billed.
- Higher A/R days: Claims slide into payer negotiation, patient disputes, or internal review.
- Preventable write-offs: Charges that should have been collected correctly at the front end become concessions later.
- Manager distraction: Owners and administrators get pulled into one-off billing escalations instead of fixing root causes.
Practical rule: If your team can't prove the correct billing pathway was triggered before a bill went out, you don't have compliance. You have exposure.
For out-of-network groups, this is even more important. If your reimbursement strategy depends on clean intake, clear notices, and defensible claim handling, weak NSA controls will undercut collections long before they trigger formal enforcement. That's why owners dealing with out-of-network reimbursement pressure should view NSA readiness as revenue protection, not paperwork.
The real cost is operational friction
In our experience, the practices that struggle aren't usually confused about the law at a high level. They know surprise billing is restricted. They know estimates matter. What they don't have is a reliable workflow from scheduling to final bill.
That gap creates compounding problems. The scheduler doesn't flag self-pay correctly. The estimate doesn't reflect actual expected services. The claim goes out with incomplete documentation. Then billing has to clean up a problem that started days earlier.
You don't solve that with a binder full of policies. You solve it by tightening front-end decisions that affect who gets billed, what can be collected, and how fast money moves.
Understanding the Core NSA Provisions
The No Surprises Act changes who you can bill, when you can bill them, and how much of the collection risk gets shifted to payer negotiations instead of patient balances.
For practice owners, the useful way to think about it is not legal theory. It's billing triggers.
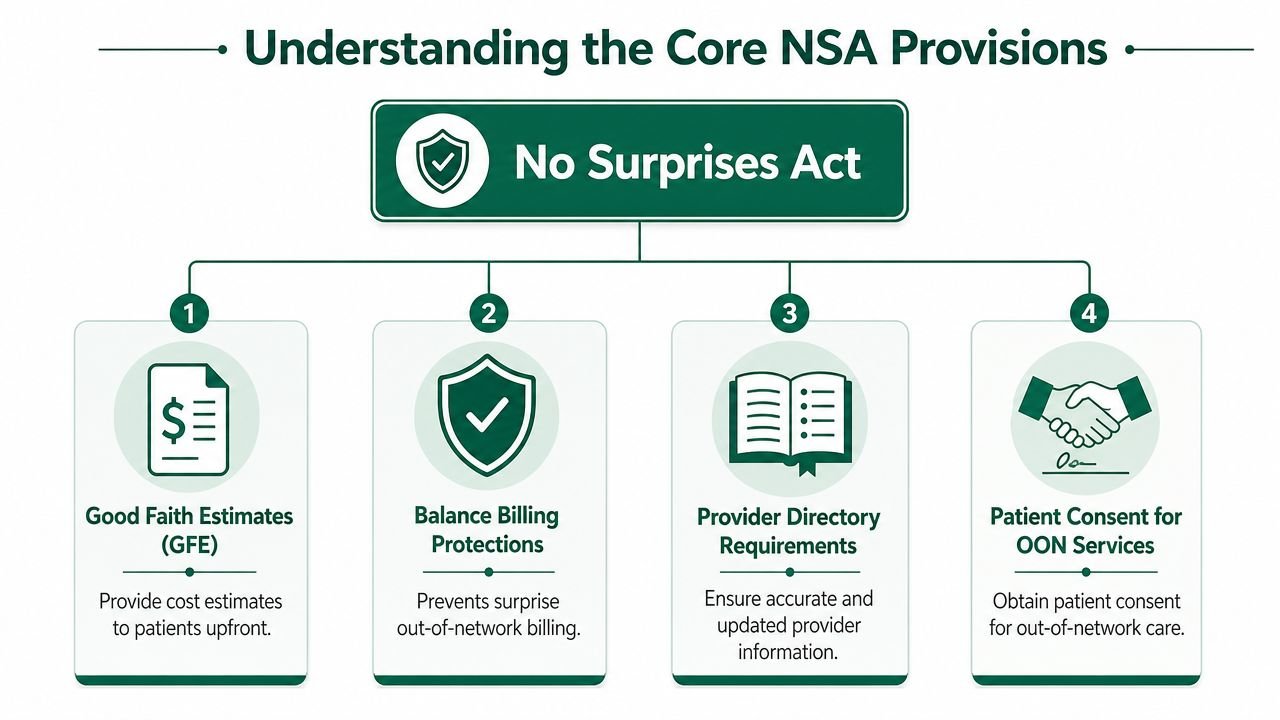
The four provisions that matter operationally
| Provision | What it changes in practice | Financial consequence |
|---|---|---|
| Balance billing protections | Limits when an out-of-network provider can bill the patient beyond in-network cost sharing | Reduces collectible patient balance in affected encounters |
| Good Faith Estimates | Requires cost estimates for uninsured or self-pay patients | Bad estimates can trigger disputes and delay payment |
| Provider directory accuracy | Bad network status information creates expectation and billing problems | Increases complaint risk and collection friction |
| Patient consent for some OON services | Consent has to be handled correctly when an exception applies | Missing or flawed consent weakens your billing position |
A common example is anesthesia. An anesthesiologist may be out of network while the facility is in network. If the encounter falls within NSA protections, your collectible amount from the patient changes immediately. That means your expected revenue on the case depends less on your fee schedule and more on whether your intake, notice, and payer process were handled correctly.
The same logic applies in specialties where ancillary services are common. Orthopedics, pain management, cardiology, GI, and hospital-based specialties all face this risk because multiple providers and service lines can touch the same encounter.
Why owners should care about adjacent policy shifts
Patient billing rules don't exist in a vacuum. If you want context on how the broader environment is changing, it's worth reviewing the impact of new medical debt rules because patient balance strategy is getting harder, not easier. That makes upstream compliance and accurate billing even more important.
If your margin depends on collecting balances you were never allowed to send, your revenue model is already broken.
What this means for day-to-day billing
Your front office and billing team need to answer three questions before a claim or statement leaves the system:
- Is this encounter protected under the NSA?
- Can the patient be billed beyond in-network cost sharing in this scenario?
- Do we have the documentation to support that decision?
If those answers aren't built into the workflow, staff will improvise. Improvisation is expensive.
Practices that also struggle with balance billing exposure usually find the same root issue. Their billing rules live in people's heads instead of in intake, eligibility, estimate, and claim-edit processes.
Mastering Good Faith Estimate Requirements
The Good Faith Estimate, or GFE, is where many practices fail first because it sits at the intersection of scheduling, pricing, coding expectations, and patient communication.
For uninsured or self-pay patients, estimates must be delivered within 3 business days of scheduling or request, and if the final charge is $400 or more above the estimate, the patient can initiate the patient-provider dispute process, as outlined in this Good Faith Estimate compliance guide.
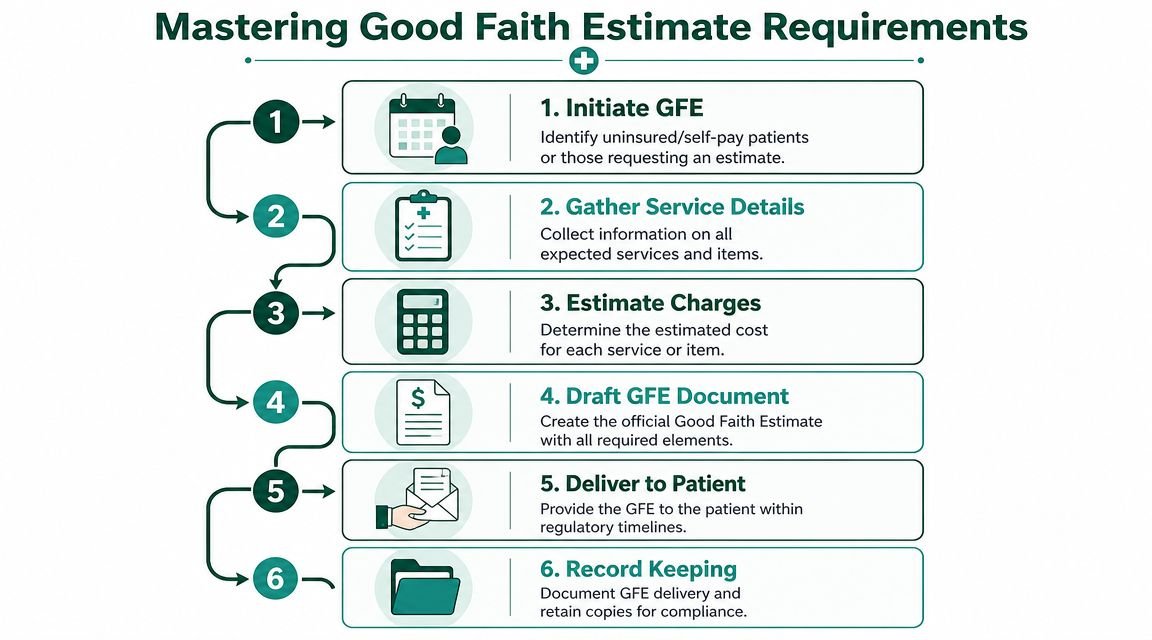
Build a GFE workflow that billing can actually defend
Most practices make one of two mistakes. They either treat the GFE like a rough courtesy quote, or they make it so manual that nobody can produce it consistently on time.
A workable process looks like this:
- Identify status at scheduling
The scheduler has to know whether the patient is uninsured, self-pay, or choosing not to use coverage. If this classification is wrong, the rest of the workflow is wrong.
Map expected services early
You don't need perfect prediction, but you do need a defensible estimate based on expected services. For procedure-heavy specialties, that may include office visit levels, imaging, injections, or follow-up services when reasonably expected.
Use actual fee schedule logic
Pull from your current chargemaster and contracted self-pay pricing rules. Don't let staff build estimates from memory.
Document delivery
If it's not timestamped and retained, assume you can't prove it happened.
Why estimate accuracy matters financially
A bad GFE doesn't just create an unhappy patient. It can stall collections and force your staff into formal dispute handling. That's why we push owners to audit high-variance services first.
For example, if your cardiology group routinely estimates a basic office workup but the actual visit includes diagnostics, or your orthopedic practice frequently underestimates bundled office-based procedures, your estimate process is not protecting revenue. It's setting up future disputes.
The right question isn't "Did we send an estimate?" It's "Could we defend the estimate against the final bill?"
Focus on your highest-risk service lines
Start with the places where service intensity changes quickly:
- Cardiology: Visits that can expand into diagnostics or imaging
- Orthopedics and pain management: Cases where injections, supplies, or imaging may be added
- Behavioral health: Session length, add-on services, and authorization-related changes
- Multi-specialty groups: Shared scheduling teams that don't understand specialty-specific charge patterns
If your specialty mix makes this hard, review specialty-specific billing workflows and compare them against your current intake and estimate process. The practices with the most GFE trouble usually have one generic script for every specialty. That doesn't work.
You should also tighten any intake process linked to surprise billing risk. The more your estimate process depends on manual follow-up, the more likely it is to fail when volume rises.
Navigating Dispute Resolution and the IDR Process
Once a billing issue moves into dispute, your advantage diminishes and your administrative burden goes up.
There are two separate tracks to understand. One involves the patient when final charges materially exceed the GFE. The other involves the provider and payer when out-of-network payment amounts can't be resolved. Owners often blur these together. They shouldn't.
Patient-provider disputes are workflow failures made visible
When a patient challenges a bill after a GFE variance, the account stops being a normal collection matter. It becomes a documentation matter.
Your team now needs to show what was estimated, when it was delivered, what services were expected, and why the final charge differed. If the chart, estimate, and billing record don't line up cleanly, you don't just face delay. You weaken your position on the receivable.
That is why front-end estimate discipline matters more than back-end argument. Once the patient is in formal dispute, the staff hours are already lost.
Provider-payer disputes create A/R drag
CMS established the federal independent dispute resolution, or IDR, framework in 2021 and issued final rules on August 19, 2022 to operationalize it. That's noted in the earlier Good Faith Estimate source, and it's the key reason owners need a clean process before claims ever reach negotiation.
In practical terms, IDR is not a healthy default operating model for a physician practice. It is a resource-intensive exception path. Every disputed out-of-network payment pulls time from your billing team, extends follow-up cycles, and complicates forecasting.
Here is the blunt version:
- If documentation is weak, you spend more time building support after the fact.
- If eligibility or encounter classification was wrong, you may be disputing a preventable payment issue.
- If claim submission quality is poor, your team enters negotiation from a weaker position.
Most practices don't have an IDR problem. They have an intake, documentation, and claim-control problem that eventually surfaces as IDR.
If you're already seeing repeat payment friction on protected out-of-network claims, review your independent dispute resolution workflow standards. The right response is usually not "hire someone to fight more disputes." It's "stop feeding avoidable accounts into the dispute track."
Keep disputes rare, not routine
Owners should ask a simple question every month. Are we entering disputes because the payer underpaid, or because our own front-end controls left room for ambiguity?
That distinction matters. One is a contracting and reimbursement issue. The other is an RCM process failure.
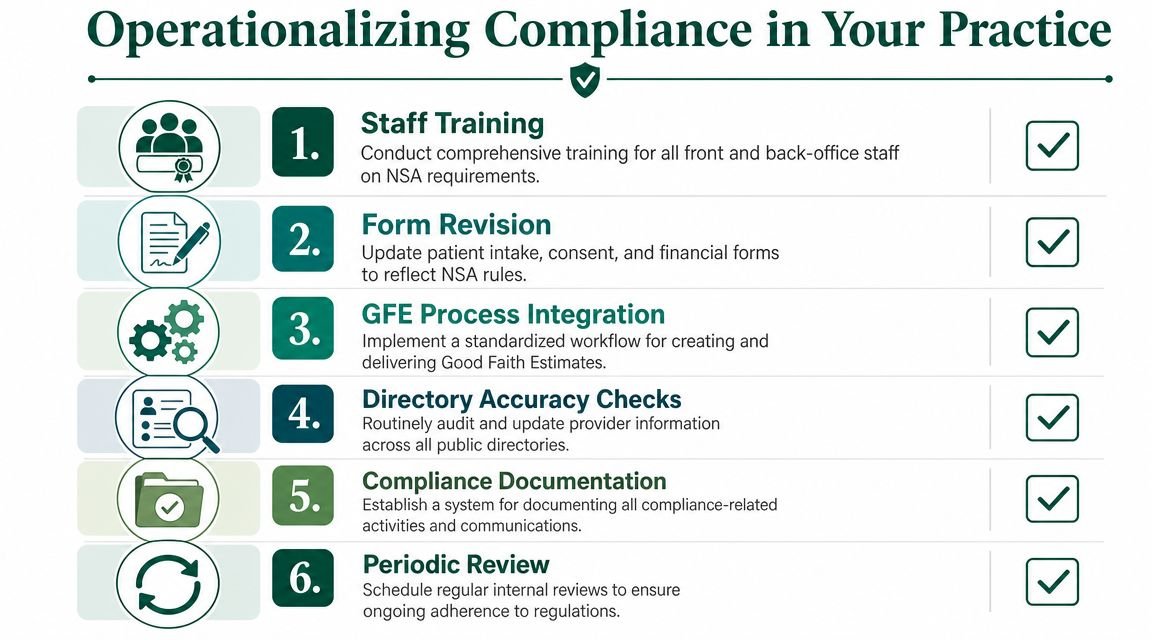
Operationalizing Compliance in Your Practice
No Surprises Act compliance lives or dies in daily operations. Policies matter. System behavior matters more.
CMS identifies three core technical obligations under the NSA: issuing GFEs for uninsured or self-pay patients, running a patient-provider dispute resolution process, and using the federal IDR process. CMS also makes the bigger point clearly. The technical risk is a control failure where the organization cannot prove the right workflow was triggered before billing occurred, as described in the CMS No Surprises Act fact sheets.
The controls you need in the system
If your EHR and practice management stack can't flag NSA-relevant encounters before charge entry or statement generation, you're relying on memory. That won't scale.
At minimum, your workflow should include:
- Real-time patient status classification: uninsured, self-pay, insured, out-of-network scenario, and protected encounter flags
- Estimate routing: automatic work queues for GFE creation and delivery tracking
- Documentation locks: stored records for notices, consent when applicable, and dispute files
- Claim edits: rules that stop staff from sending patient balances that should not go out
- Exception reporting: daily review of encounters with missing estimate or notice documentation
This is also where call handling matters. If your front desk or contact center gives inconsistent answers about network status, self-pay expectations, or estimated cost, they create downstream collection problems. Teams reviewing broader contact center compliance guidelines will recognize the same principle. Scripts, escalation paths, and documentation standards reduce avoidable risk.
Train staff on trigger points, not legal theory
Most training is too abstract. Staff don't need a lecture on federal policy. They need to know what to do when a patient schedules, asks for an estimate, declines to use insurance, or questions a bill.
Use role-based training:
| Role | What they must recognize | What happens if they miss it |
|---|---|---|
| Scheduling | Uninsured or self-pay trigger | No GFE workflow starts |
| Front desk | Network and payment expectation mismatch | Patient receives wrong financial message |
| Billing | Protected encounter and statement suppression rules | Prohibited billing goes out |
| Management | Variance and dispute trends | Root causes stay hidden |
Manual workarounds are the real threat
We've seen practices with solid written policies still fail because the software couldn't stop a prohibited bill from being generated. That's the central point. No surprises act compliance is not a policy shelf item. It's a sequence of system-enforced decisions.
If your team is using spreadsheets, sticky notes, or individual inbox reminders to manage estimates and dispute readiness, you already have a control gap. That gap usually surfaces as rework, denials, or avoidable patient balance reversals.
If you're not sure where those breaks are happening, get an RCM audit of your current workflow. A good audit should trace the encounter from scheduling through billing and show exactly where NSA controls are failing.
Auditing and Monitoring Your NSA Compliance
If you don't measure this, you'll find problems only after revenue is already delayed.
The most useful NSA audit is not a legal checklist. It's a management dashboard tied to intake quality, estimate accuracy, payer response timing, and dispute volume. Timing matters here. Guidance summarized by industry sources notes that payers must make an initial payment or denial within 30 days of a clean claim, and that automated estimation only works when chargemasters are accurate and billing systems flag NSA-applicable scenarios before a claim is sent, according to this NSA workflow summary.
Audit the process in this order
Start with a sample of recent encounters that should have triggered NSA-related workflows. Then review them backward from final bill to scheduling.
Check for:
- Correct patient classification: Was the patient identified properly at intake?
- Estimate evidence: Was a GFE required, and if so, can you prove it was sent?
- Charge consistency: Did the final billed services broadly align with what was expected?
- Claim readiness: Did claim edits catch missing documentation before submission?
- Statement controls: Did the system prevent patient billing where it should have?
Audit what the system did, not what staff say they usually do.
NSA compliance KPIs for practice owners
| KPI | What It Measures | Target | Financial Impact if Target is Missed |
|---|---|---|---|
| GFE timeliness | Whether required estimates are sent within the required window | Full compliance with required timelines | Late estimates increase dispute risk and delay collections |
| GFE-to-final-bill variance | How closely estimates match actual charges | Low and explainable variance | High variance creates patient disputes and write-off pressure |
| NSA flag accuracy | Whether eligible encounters are correctly identified | High accuracy with minimal manual correction | Misclassification leads to billing errors and rework |
| Clean claim speed on NSA-relevant accounts | Whether protected or disputed scenarios are submitted cleanly | Fast submission with minimal edits | Slower claims increase A/R days and payer friction |
| Patient dispute volume | How often GFE or billing disagreements escalate | Rare and trending downward | More disputes consume staff time and hold revenue |
| IDR case volume | How often provider-payer negotiations escalate formally | Reserved for true exceptions | Frequent escalation signals weak front-end controls |
The exact target thresholds will vary by specialty and operating model, but the pattern should be clear. If estimate variance rises, disputes usually follow. If classification errors rise, claims and statements become unstable.
Use NSA monitoring to improve core RCM
A good compliance review also tells you whether your broader revenue cycle is healthy. Practices that monitor estimate quality, intake accuracy, and clean-claim discipline usually improve more than compliance. They tighten collections, reduce avoidable follow-up, and get cleaner visibility into where money is being lost.
If you need a baseline, use a structured revenue cycle management checklist and layer NSA checkpoints into your existing monthly review.
Frequently Asked Questions About NSA Compliance
Does the No Surprises Act only matter if my practice is out of network
No. Out-of-network practices feel the pressure differently, but in-network groups still face NSA workflow risk through scheduling, estimates, ancillary services, and patient communication. If your staff mishandles a protected encounter or a self-pay estimate, you can still end up with delayed revenue and avoidable disputes.
What's the biggest operational mistake physician practices make
They assume billing can fix what scheduling failed to classify. It can't. If the patient wasn't identified correctly at intake, the estimate wasn't generated properly, or documentation wasn't retained, your billing team is cleaning up a control failure after the fact.
Should my front desk be responsible for NSA compliance
Your front desk should be responsible for trigger recognition, not for interpreting the law. They need clear scripts and hard workflow rules for uninsured status, self-pay requests, network questions, and estimate routing. Management and billing should own oversight and exception review.
Can we handle this with manual spreadsheets and reminders
You can for a short time. You shouldn't for long. Manual tracking breaks when volume rises, staff turns over, or one person gets overloaded. If a workflow affects whether a patient can be billed and whether revenue gets delayed, it belongs inside the system with reporting and accountability.
No Surprises Act compliance is a revenue discipline disguised as a regulatory one. Owners who treat it that way usually reduce rework, protect collections, and keep A/R from drifting upward. Owners who don't usually discover the problem one disputed bill at a time.
If your practice is dealing with estimate errors, balance billing confusion, rising denials, or slower collections, Happy Billing can help you find the breakdown fast. We work inside existing practice workflows to identify where intake, claim edits, and patient billing controls are leaking revenue. If you want a clear view of what your current process is costing you, request a free RCM audit.