Optimizing Wound Care Billing Services for 2026
Wound care billing services exist to stop one of the worst revenue leaks in physician billing. In this specialty, denial rates often exceed 15 to 20% without specialized expertise, and practices that adopt specialized protocols can increase revenue by 10 to 20% while pushing denials into single digits.
This is the core issue. This isn't about outsourcing a back office task. It's about whether your practice keeps losing reimbursable wound revenue because your current billing team treats wound care like ordinary office billing.
Wound care claims fail for predictable reasons. Surface area is documented vaguely. Depth isn't stated clearly enough to support the higher-paying code family. An E/M is billed on the same day as a procedure without the right modifier. A biologic is billed without a defensible documentation trail. Then your staff spends weeks chasing avoidable denials while A/R ages and cash flow tightens.
A specialized wound care billing service is a revenue protection function. It combines documentation review, code selection, modifier logic, payer-rule checks, and denial prevention into one workflow built around wound care's unusually strict claim requirements. In our experience, practice owners usually don't have a collections problem. They have a precision problem.
Why Standard Billing Fails at Wound Care
Generic billing teams usually break down at the exact point wound care becomes financially sensitive. They know how to post charges. They don't always know how to defend a wound claim before it ever reaches a payer.
That matters because wound care has one of the highest denial rates in medical billing, often exceeding 15 to 20% for practices without specialized expertise, while specialized protocols can raise revenue by 10 to 20% and reduce denials to single digits, according to this wound care billing analysis. If your practice is still routing these claims through a generalist workflow, you're probably leaking revenue every week.
The problem isn't volume. It's precision.
Most practice owners assume denials happen because payers are difficult. Payers are difficult. But in wound care, they're also consistent. They deny when documentation is incomplete, inconsistent, or too vague to support the billed service.
The weak points show up fast:
- Measurement gaps: Notes don't include exact wound dimensions in centimeters and total cm².
- Progression gaps: The chart doesn't clearly show whether the wound improved, stalled, or worsened.
- Procedure mismatch: The note supports one level of service, but the claim reflects another.
- Modifier failure: Same-day services get bundled because the billing team didn't apply the right modifier logic.
Standard billing departments react after the denial. Specialized wound care billing services prevent the denial upstream.
What practice owners should take from this
If your denial rate is high, wound care is not the place to “clean things up later.” Every rejected claim creates more work, more appeal lag, and more pressure on cash flow.
A good starting point is to compare your current process against common medical billing company red flags. If your vendor can't explain how they validate wound measurements, same-day E/M billing, and payer-specific bundling before submission, they're not running a wound care workflow. They're running a generic claims shop.
The Anatomy of a Specialized Wound Care Billing Workflow
A specialized wound care billing workflow doesn't begin with claim submission. It begins before the claim exists. The goal is to catch defects while the note can still be fixed, not after the payer has already denied the encounter.
The strongest wound care billing services build a sequence that connects clinical documentation, coding logic, and payer edits in near real time.
What happens before the claim goes out
First, the service reviews the wound note for billing-critical details. That includes exact dimensions, depth, stage, drainage, and exposed structures when relevant. If those elements are unclear, the claim should not move forward as if the documentation is good enough. That's how avoidable denials get created.
Second, the coding team checks whether the documented treatment supports a surface-area-based code or a depth-based debridement code, a common point of financial loss for generalist teams. They either undercode to stay “safe” or overcode without enough support, which is worse.
Third, the service checks same-day service combinations against CCI edits and payer bundling rules. This is especially important when an E/M and a procedure occur in the same visit.
What a real specialist does differently
A real specialist doesn't wait for the ERA to reveal a problem. They audit logic before submission.
That workflow usually includes:
- Documentation validation: Confirm the note supports the code family being selected.
- Modifier review: Check whether modifier -25, -59, -LT, or -RT is required based on the encounter.
- Claim scrubbing against payer edits: Catch bundling, incompatibility, or support issues before submission.
- Fast feedback to the practice: Send documentation queries while the visit is still recent and fixable.
According to this wound care billing guide, organizations using 24/7 follow-the-sun workflows verify each modifier placement against CCI edits and payer-specific bundling rules within hours of service entry, preventing denials that would otherwise take 15 to 20 business days to appeal. That speed matters because the longer a bad claim sits, the more expensive it becomes to recover.
Practical rule: If your billing partner only talks about denial management, ask what they do in the first 24 hours after the encounter. That's where most wound care revenue is either protected or lost.
Why this workflow improves cash flow
Practice owners should care about one thing here. Time to cash.
A specialized workflow shortens the distance between documentation and reimbursement because it reduces the number of claims that need rework. It also lowers the number of provider queries that happen too late, when nobody remembers the encounter well enough to fix the note cleanly.
That's why wound care billing services should be judged less by how many claims they “process” and more by how aggressively they prevent weak claims from leaving your system in the first place.
Common Coding and Documentation Pitfalls Costing You Thousands
A single wound care documentation mistake can turn a properly payable encounter into a lower-paid code, a bundled line item, or a full denial. That is the core financial problem.
Wound care billing is unforgiving because reimbursement depends on details many general billing teams miss. Measurement drives add-on coding. Tissue depth drives code family selection. Modifier logic determines whether separate work gets paid or written off. According to this guide to wound care billing codes, CPT 97597 covers the first 20 sq cm of selective debridement, +97598 is used for each additional 20 sq cm, and the 11042 to 11047 code family applies to surgical debridement based on tissue depth. The same source notes that missing or vague wound dimensions are a common reason claims fail.
Here is what that means in real money.
If the provider documents debridement but fails to state the tissue depth clearly, the billing team often drops to the lower-paying code set because the chart cannot defend surgical debridement. If a wound measures beyond the base threshold but the note does not support total area, the add-on code never gets billed. If the physician performs a separately identifiable E/M service on the same day and the claim goes out without modifier -25, the payer often bundles it into the procedure and keeps the extra reimbursement.
These are not abstract coding errors. They are recurring write-offs built into your workflow.
The mistakes that drain revenue
The first leak is depth ambiguity. Debridement to subcutaneous tissue, muscle, or fascia must be documented at that level. If the note says only “debridement performed,” your team cannot defend the higher-value surgical code family.
The second leak is incomplete measurement. “Large wound” has no billing value. You need length, width, and total surface area documented clearly enough to support the base code and any add-on units.
The third leak is modifier failure. Wound care claims regularly require judgment about whether services were distinct, separately identifiable, or subject to bundling edits. A generalist billing team often treats modifier use like cleanup. A specialized team treats it like revenue protection.
The financial impact of common wound care coding errors
| Common Error | Correct Code/Modifier | Typical Revenue Lost Per Claim | Prevention Strategy |
|---|---|---|---|
| Depth not documented, so surgical debridement can't be supported | 11043 when muscle/fascia is explicitly documented | Higher-level debridement may be downcoded to a lower-paying service | Require explicit tissue-depth documentation in the note |
| Additional wound area not captured | +97598 for each additional 20 sq cm | Add-on reimbursement is missed when only the base code is billed | Document exact length, width, and total cm² every visit |
| Same-day E/M billed without -25 | E/M with modifier -25 plus procedure code | Payer bundles the E/M into the procedure | Review same-day E/M documentation before claim submission |
| Distinct procedures billed without separation logic | -59 or anatomical modifiers such as -LT and -RT when supported | Claim lines are denied or combined under CCI edits | Check procedure combinations against payer edit rules before release |
| Wound described vaguely | Correct area-based or depth-based code family | Claim support is weak, which raises denial and downcoding risk | Standardize note templates and measurement capture |
What specialized billing fixes that standard billing misses
A specialized wound care billing service does not just code what shows up in the chart. It checks whether the chart supports the highest defensible reimbursement before the claim leaves your system. That means reviewing wound measurements, confirming tissue depth, validating modifier logic, and querying the practice while the visit is still fresh enough to correct.
That process gets even more important when records are fragmented across progress notes, procedure notes, and images. Practices that streamline medical record reviews give their billing team a better shot at catching missing support before submission. Without that discipline, staff either underbill to stay safe or submit claims that collapse on review.
The best billing partners now use a hybrid AI and human review model. AI flags missing measurements, inconsistent depth language, and likely modifier issues across large claim volume. Experienced wound care billers then verify payer rules, clean up edge cases, and send targeted documentation queries. That is how you stop losing money one encounter at a time.
If you want a clearer view of where these failures start, this guide to medical billing complexities explained breaks down the operational weak points that wound care exposes faster than almost any other specialty.
The expensive mistake is not the denial itself. The expensive mistake is sending a claim that never had the documentation to earn full payment.
Proactive Denial Prevention for Wound Care Claims
Most wound care denials aren't solved by becoming more aggressive after the remittance arrives. They're solved by building claims that can survive scrutiny the first time.
That means thinking beyond CPT selection. The claim has to show why the service was necessary, why the frequency was appropriate, why the wound status justified continued treatment, and why any advanced product or supply billing was compliant with payer rules.
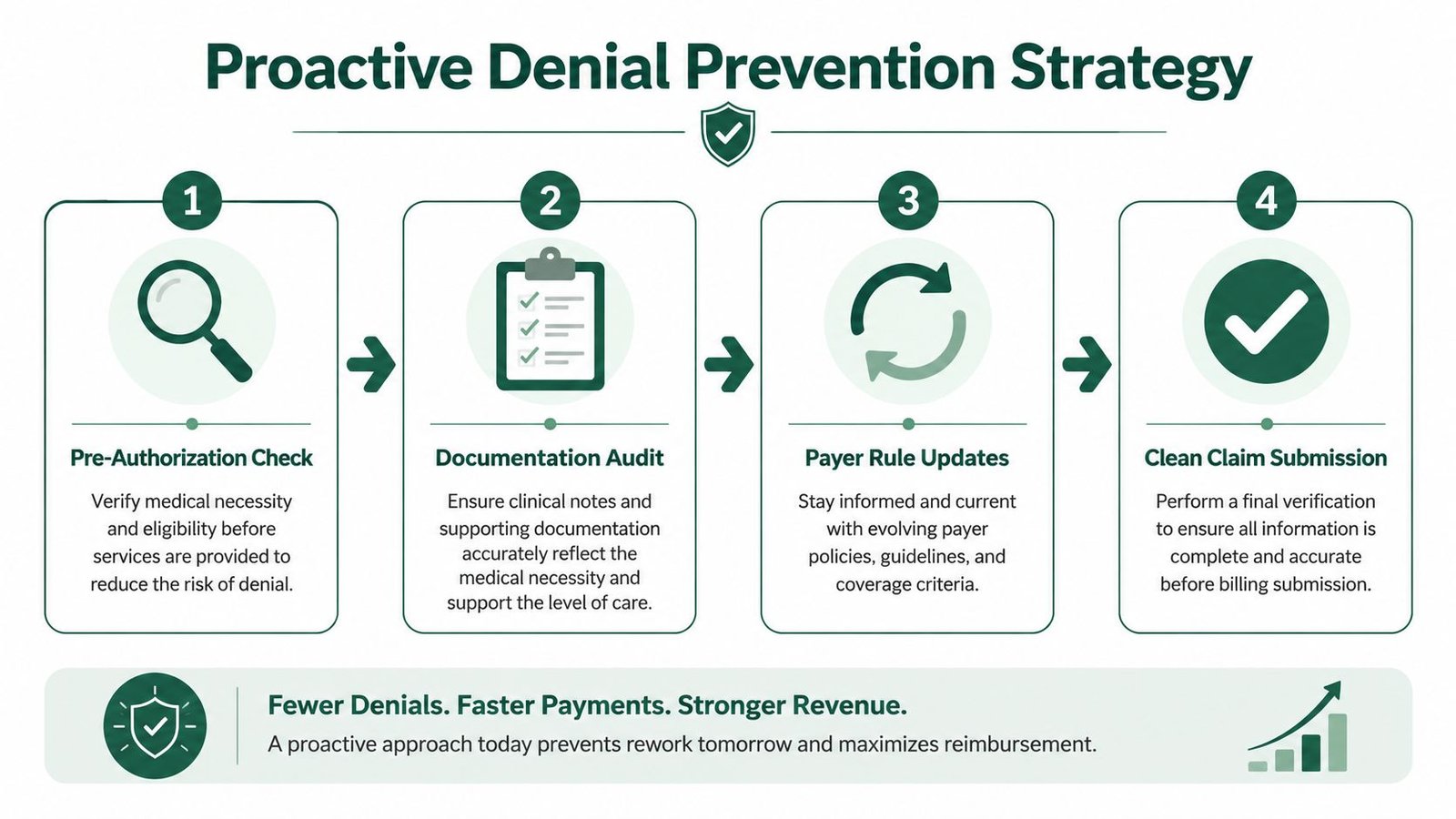
Build a defensible claim, not just a coded claim
The strongest wound care billing services treat every recurring wound episode like a payer audit waiting to happen. They don't assume medical necessity is obvious. They prove it through the chart.
That usually requires:
- Progress tracking: Each visit should show whether the wound improved, plateaued, or deteriorated.
- Treatment rationale: The note should explain why the selected intervention was clinically appropriate at that stage.
- Frequency support: Repeated services need documentation support, not repetition by habit.
- Supply logic: Advanced products need a clean connection between the clinical record, HCPCS billing, and payer rules.
Advanced supplies are where many groups get burned
Biologics and advanced wound supplies create another layer of risk because reimbursement is tightening and bundling rules are complicated. According to this wound care billing services overview, OIG reports show compliant practices using layered HCPCS Q-code stacking with E/M modifiers can recover up to 22% more revenue on these high-cost biologics.
That doesn't mean bill more aggressively. It means bill correctly, with enough support to avoid audits and underpayment.
If your group uses biologics, ask three hard questions:
- Are Q-codes being matched to the chart with documentation that supports use and medical necessity?
- Is the E/M on the same day distinct and billed accordingly?
- Does your team know when the payer will bundle the product versus reimburse separately?
A denied biologic claim is worse than a denied routine procedure claim. The dollars are higher, the audit exposure is higher, and the appeals burden is heavier.
Owners dealing with recurring denials in this area should also review how medical billing denial management works at the process level. If your current vendor treats every denial the same, they're not protecting wound care revenue correctly.
Measuring Performance and ROI for Specialized Billing
A small drop in wound care claim performance can erase more profit than a billing fee ever will. If your team misses documentation details that trigger denials, the loss shows up per encounter, then again in rework labor, slower cash, and preventable write-offs.
Start with the metrics tied directly to cash. Fee percentage is secondary.
The metrics that show whether your billing partner is protecting revenue
Review these every month, and review them specifically for wound care, not blended across all specialties:
First-pass reimbursement rate
This shows how many claims get paid without rework. If this number slips, your practice is paying staff to touch the same dollars twice.Net collection rate
This tells you how much of your allowed revenue reaches the bank. A weak number means earned revenue is leaking out after the visit.Denial rate
This is your early warning sign. In wound care, rising denials usually point to failures in measurement capture, modifier use, medical necessity support, or payer-specific edits.A/R days
This measures how fast revenue turns into cash. High A/R days choke cash flow and force owners to fund payroll and supplies while insurers sit on money already earned.
If you want a broader view on how smart operators choose metrics that drive decisions, this article on choosing KPIs for startup growth makes the right point. Track numbers you can act on.
What specialized billing ROI actually looks like
A specialized wound care billing service should improve four financial outcomes at the same time:
- More claims paid on the first submission
- Fewer dollars trapped in denials and appeals
- Faster payment velocity
- Less staff time wasted fixing preventable errors
That is the ROI.
Use a simple formula:
Recovered revenue + avoided write-offs + reduced rework cost – billing partner cost = net financial gain
Keep it practical. Compare your numbers from the 90 days before the billing change against the 90 days after implementation. Then review the difference by wound care encounter volume, denial category, and payment speed.
| KPI | What strong performance looks like | What weak performance usually means |
|---|---|---|
| First-pass reimbursement rate | High and stable over time | Claims leave with preventable coding or documentation errors |
| Net collection rate | Consistently close to allowed revenue | Your practice is doing the work but not collecting the full value |
| Denial rate | Low and trending down | Front-end edits are weak and preventable denials are reaching payers |
| A/R days | Low and controlled | Follow-up is slow, appeals stall, or claims are aging unnecessarily |
Translate those KPIs into dollars
Owners get clarity fast.
If a denial delays payment on a wound care claim, you are not just waiting on cash. Your team is spending more labor to correct the claim, resubmit it, track it, and appeal it if needed. Multiply that by recurring documentation mistakes and your margin gets thinner every month.
A specialized partner fixes that by combining rules-based automation with experienced wound care billers. The AI layer flags missing measurements, modifier conflicts, and payer edit risks before submission. The human layer reviews chart context, validates coding logic, and stops bad claims from leaving the system. Generic billing shops usually stop at basic scrubbing. That is not enough for wound care.
If your reporting still lives in static month-end summaries, fix that first. Practice owners need medical billing KPIs to track in a format that shows where revenue is leaking, which denial reasons are rising, and whether the billing partner is improving cash performance.
Judge the vendor by financial movement. If first-pass performance improves, net collections rise, and A/R days tighten, the service is paying for itself. If those numbers do not move, you are funding overhead, not buying results.
How to Evaluate a Wound Care Billing Partner
Most vendors will tell you they “do wound care.” That claim means nothing unless they can show how they prevent wound-specific leakage before claim submission.
You're not hiring a vendor to post charges. You're hiring a partner to protect difficult revenue.

Questions that separate specialists from generalists
Ask every prospective partner these questions:
What is your wound care first-pass performance?
Don't accept broad company-wide numbers if they can't explain wound-specific workflows.How do you validate wound measurements and depth before submission?
If they answer with generic “claim scrubbing,” keep pushing. You want to hear how they handle exact dimensions, tissue depth, and same-day procedure logic.How do you manage modifier decisions for E/M plus procedures?
They should be comfortable talking through -25, -59, -LT, and -RT in practical terms.What do you do when documentation is incomplete?
The right answer is not “we submit and appeal if needed.”How do you work inside our current EHR?
A good partner should reduce friction, not create a migration project.
What a serious partner should be able to show you
A strong vendor should be willing to walk you through:
- A sample pre-submission review process.
- A denial trend report for wound claims.
- Their escalation path for documentation deficiencies.
- How they handle specialty overlap in settings like orthopedics, dermatology, or pain management.
That last point matters. Many wound encounters originate inside broader specialty workflows. If you're evaluating partners with cross-specialty needs, review their broader specialty billing capabilities and their approach to outsourced revenue cycle management. A vendor that understands only one narrow slice of your revenue cycle usually creates handoff problems somewhere else.
If a billing company can't explain where wound claims fail before submission, they won't fix the problem after denial either.
Frequently Asked Questions From Practice Owners
Should we train our in-house team or move to specialized wound care billing services
Train internally only if your team already catches wound-specific revenue loss before the claim goes out. That means accurate measurements, procedure-to-documentation matching, modifier discipline, and payer-specific edit control. If those checks are inconsistent, every missed detail turns into underpayment, denial work, or write-offs.
For many practices, specialized wound care billing is the cheaper option. A preventable denial does not just delay cash. It adds staff rework, provider chart corrections, appeal time, and slower collections. A specialist fixes the front end so each encounter has a better chance of paying correctly the first time.
How disruptive is implementation if we switch billing partners
A good transition should be operational, not chaotic. The partner should map your current workflow, identify where documentation breaks down, configure payer edits, and set a reporting cadence your team can practically use.
If implementation turns into a long technology project, the vendor is solving the wrong problem. Wound care billing services should fit your existing EHR and tighten claim quality without creating new friction for providers.
What's the real difference between a general medical billing company and a wound care specialist
The difference is paid revenue per encounter.
A general billing company can enter charges and submit claims. A wound care specialist reviews whether the wound dimensions support the code, whether the depth documented matches the procedure billed, whether the same-day E/M supports modifier use, and whether supply capture is being missed. Those are not technical details. They determine whether you get paid in full, paid late, or not paid at all.
The best services use a hybrid AI and human workflow. AI flags missing measurements, inconsistent tissue descriptions, modifier conflicts, and payer edit risks before submission. Experienced wound billing staff then review those exceptions, correct what can be fixed, and send documentation issues back before they become denials. That model protects revenue better than either automation alone or manual billing alone.
How quickly should we expect financial improvement
You should see leading indicators early. Fewer front-end documentation defects. Fewer preventable denials. Faster claim acceptance. Cleaner reporting on where money is leaking.
Meaningful revenue improvement follows once those errors stop repeating and aged claims start clearing. If a billing partner cannot show those operational changes quickly, do not expect a delayed financial miracle.
If your wound care claims are being denied, underpaid, or aging out, the problem is usually process accuracy tied directly to dollars lost per visit. Happy Billing helps physician groups tighten that process with specialty-specific RCM, hybrid AI and human claim review, and workflows built to reduce leakage without forcing an EHR migration. If you want a precise picture of where your practice is losing revenue, book a free billing audit.