Master Telehealth Billing for Mental Health: A Code-Level Guide
To master telehealth billing for mental health, your practice must correctly bill a trio of codes on every claim: the appropriate CPT code (like 90834), a Place of Service (POS) code of 10 (for patients at home), and Modifier 95 (for synchronous audio/video). This combination is non-negotiable for most payers, including Medicare, and getting it wrong is the leading cause of preventable telehealth denials. This guide provides the specific codes and payer rules practice managers need to ensure a clean claim rate.
This isn’t just about ticking boxes; it’s the foundation for a healthy revenue cycle in the new era of virtual care. Let's walk through the operational plan to get it right every time.
The New Reality of Mental Health Billing

Telehealth is no longer a temporary fix—it's a core part of your practice. For many mental health providers, virtual sessions now make up anywhere from 30% to 60% of all patient appointments. What started as a crisis response is now a permanent—and profitable—care model.
The operational wins are undeniable. Offering sessions at home can slash no-show rates by up to 30% and boost clinician capacity by as much as 40%. But these benefits evaporate if your billing workflows aren’t built for telehealth-specific rules. You can find a complete breakdown of these efficiencies in our guide to mental health revenue cycle management.
Medicare cemented this shift by extending its key telehealth flexibilities through December 31, 2024. This gives your practice the stability to invest in long-term virtual care strategies, but it comes with strings attached.
The In-Person Mandate You Can't Ignore
Here’s the biggest tripwire in the new Medicare rules: the in-person visit mandate. For a patient to be eligible for ongoing telehealth services, they must have an in-person visit:
- Within the six months before their first telehealth appointment.
- At least once every 12 months thereafter.
For practice managers, this means your scheduling and EMR workflows must now track this 12-month look-back period for every telehealth patient. The goal is to weave these required visits into the care plan without disrupting the flow of virtual therapy.
Fail to track this, and claims will be automatically denied. A telehealth session billed in month 13 without a documented in-person visit in the prior year is dead on arrival.
The Financial and Operational Stakes
The good news is that this long-term stability from CMS allows practices to confidently invest in the technology and training that virtual care demands. This is especially critical for providers serving in Mental Health Professional Shortage Areas (HPSAs), where telehealth is a lifeline.
Here’s a quick reference table to make sure your claims have the right DNA.
Core Telehealth Billing Components for Mental Health Claims
This table breaks down the essential coding elements your team needs to get right on every telehealth claim. Think of it as your pre-submission checklist to prevent easy-to-fix denials.
| Billing Component | Code/Value | Description & Common Use Case |
|---|---|---|
| CPT Code | 90834, 90837, etc. | The service provided (e.g., a 45-minute or 60-minute psychotherapy session). This code remains the same as for an in-person visit. |
| Place of Service (POS) | 10 | Indicates the patient was located at their home. This is the new standard for telehealth and replaces the old POS 02 for most payers. |
| Modifier | 95 | Signals that the service was delivered via synchronous (real-time) audio and video. This modifier is critical for most commercial and federal payers. |
Using these three components correctly is the bedrock of a high clean claim rate for telehealth. It tells the payer exactly what happened, where it happened, and how it happened.
Your key operational takeaways should be:
- Standardize Your Billing Template: Every telehealth claim must be built with the CPT code + POS 10 + Modifier 95 structure. No exceptions.
- Integrate In-Person Visit Tracking: Your EMR or practice management system needs a mechanism to flag patients approaching their 12-month in-person visit deadline.
- Always Verify Payer Rules: While CMS sets the tone, commercial payers often have their own subtle variations. Telehealth policy should be a mandatory part of every eligibility check.
Mastering these workflows isn't just about avoiding denials. It's about future-proofing your practice's revenue and securing your ability to deliver care, no matter where your patients are.
Mastering CPT Codes and Modifiers for Telehealth Sessions
Getting telehealth billing right comes down to precision. Your claim is a story, and every detail—the CPT code, the place of service, the modifier—must be perfect to get paid. Think of it less as paperwork and more as the primary driver of claim acceptance. Without it, you’re just doing free work.
The core of tele-mental health billing is built on just a few psychotherapy codes. But the real trick is knowing which one to pick based on the documented session time. That’s where most of the money is won or lost.
Core Psychotherapy CPT Codes for Telehealth
The CPT codes for telehealth are the same ones you use for in-person visits. The difference is that for virtual sessions, payers scrutinize your time documentation. Your session notes are your only defense in an audit.
These are the codes your practice will live and breathe by:
- CPT 90832: Psychotherapy, 30 minutes (use for sessions between 16-37 minutes).
- CPT 90834: Psychotherapy, 45 minutes (use for sessions between 38-52 minutes).
- CPT 90837: Psychotherapy, 60 minutes (use for sessions 53 minutes or longer).
The line between CPT 90834 and 90837 is a common tripwire. Bill a 50-minute session as 90834, and you’re fine. Bill it as 90837, and you’re asking for a denial. Your clinical notes must explicitly state the session "start time" and "end time" to back up your code selection.
For practices looking to get every dollar they’ve earned, mastering the difference is non-negotiable. We break it down further in our guide to billing with CPT 90837 vs 90834.
Applying the Correct Modifiers and Place of Service
Picking the right CPT code is just step one. You also have to tell the payer how you delivered the service. This is where a single mistake can trigger an immediate rejection.
For almost all real-time audio and video telehealth sessions, the rules are thankfully becoming standardized.
- Modifier 95: This is the industry standard for a synchronous telemedicine service. It’s recognized by Medicare and the vast majority of commercial plans.
- Place of Service (POS) 10: This code confirms the patient was at home during the virtual session. Don't use the old POS 02 code—it's a guaranteed denial.
Billing Example: A 50-minute psychotherapy session held over a HIPAA-compliant video call with a patient at home should be billed like this: CPT 90834 + POS 10 + Modifier 95.
While Modifier 95 is king, you might still run into payers that cling to old habits, like requiring a proprietary modifier such as GT. This is becoming rare, but it’s exactly why your front-office team needs to confirm telehealth rules during every eligibility and benefits check. One quick call can save you weeks of chasing a denied claim.
Billing for Specialized and Crisis Services
Your telehealth billing isn't just for routine 45-minute therapy sessions. More intensive services, like initial intakes and crisis interventions, are also fully reimbursable when coded correctly.
The psychiatric diagnostic evaluation is one of the most common and important services you'll bill.
- CPT 90791 (Psychiatric Diagnostic Evaluation): This code is widely covered for telehealth. Just like a standard session, you’ll bill it with POS 10 and Modifier 95. Be warned: 90791 often requires prior authorization, so your intake workflow should automatically flag it for verification.
When urgent situations arise, you can also use crisis psychotherapy codes for virtual appointments.
- CPT 90839 (Psychotherapy for crisis; first 60 minutes): This code is for urgent assessments when a patient is in crisis. For telehealth, bill it with POS 10 and Modifier 95. Your documentation must paint a clear picture of the crisis—mentioning the patient's acute condition (e.g., severe suicidal ideation, acute psychosis) and the steps you took.
- CPT +90840 (Add-on code for each additional 30 minutes): This is an add-on code, used with 90839 when a crisis session goes beyond the first 60 minutes.
Properly coding these specialized services ensures you get paid for the full spectrum of care you provide. Getting telehealth billing right demands a disciplined, almost obsessive approach to codes, modifiers, and time-based documentation.
Navigating Payer-Specific Telehealth Rules
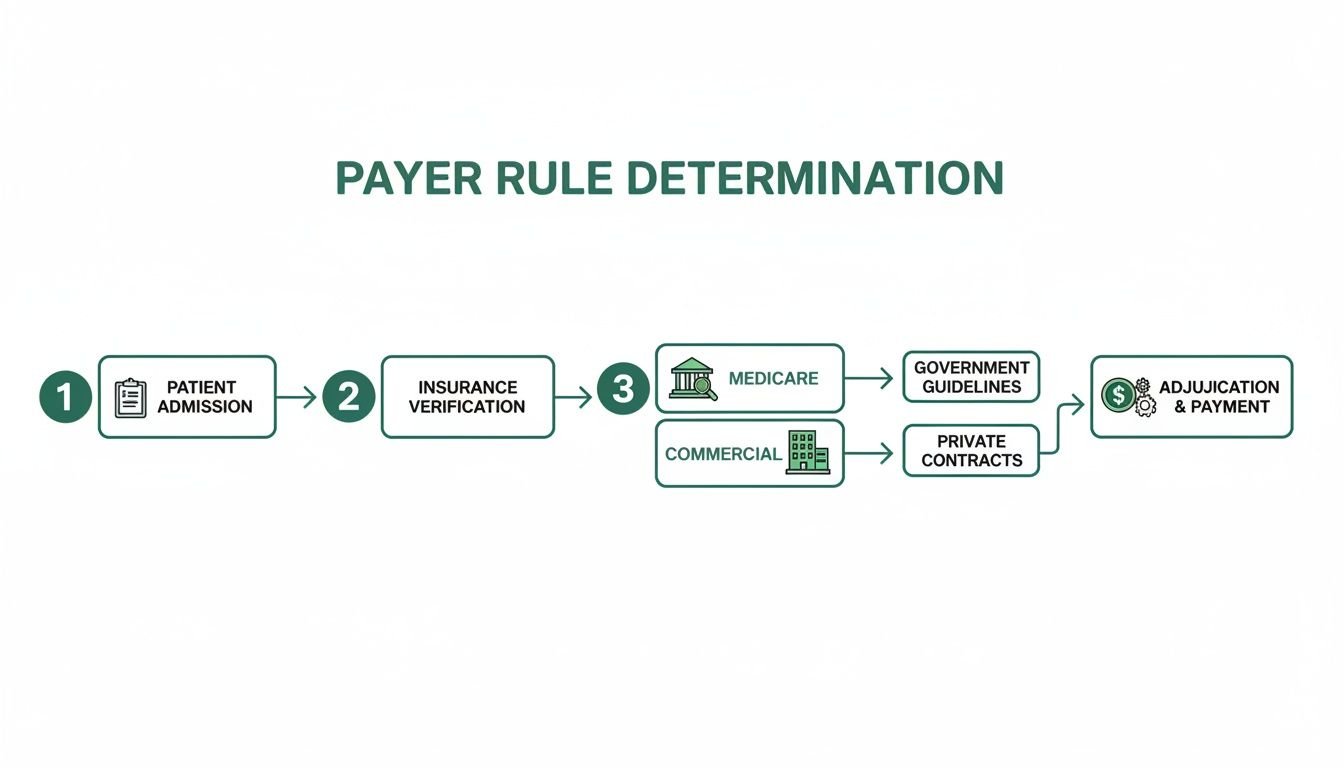
Getting your CPT codes and modifiers straight is a solid start, but it’s only half the job. The real challenge in telehealth billing is cracking the code of each individual payer’s rulebook. While Medicare sets a national direction, commercial giants like UnitedHealthcare, Aetna, and Cigna all march to the beat of their own drum.
Your practice's financial health depends entirely on how well you can map, track, and follow these constantly shifting policies. It can feel like you’re chasing a moving target. The trick is to stop looking for a single "telehealth rule" and start building a payer-specific playbook. What gets a Medicare claim paid will often trigger an instant denial from a commercial plan that demands a different modifier or has its own unique authorization quirks.
Medicare: The Payer Setting the Pace
When it comes to telehealth, everyone watches Medicare. Their decisions almost always trickle down to commercial payers, and right now, they’ve given behavioral health a clear runway through the end of 2024. This is a huge deal. It removes the “telehealth cliff” anxiety and provides the stability needed to build sustainable virtual care programs.
The key takeaway from the current CMS guidelines is that behavioral health is the major exception to the geographic and originating-site restrictions that have snapped back into place for other specialties. This is great news, but it comes with a critical string attached: the in-person visit mandate.
For any ongoing behavioral telehealth services, Medicare requires the patient to have at least one in-person visit with a provider from your practice within the previous 12 months. If you can't prove that visit happened, the claim will be automatically denied. No questions asked.
The Behavioral Health Exception and HPSAs
One of the most powerful parts of Medicare's current policy is the total removal of geographic barriers for behavioral health. Before, telehealth was mostly restricted to patients in rural or officially designated underserved areas. Now, for mental health services, those walls are gone.
This is a game-changer for practices looking to expand their reach, especially into Health Professional Shortage Areas (HPSAs). Right now, more than 120 million Americans live in communities with inadequate access to mental healthcare. Your practice can now offer vital tele-mental health services to these patients no matter where they are, without worrying about the old "originating site" rules.
This isn't just a billing update; it's a strategic opportunity. You can grow your patient base significantly while filling a massive public health need. It transforms telehealth from a convenience into a primary tool for bridging the healthcare gap.
How Commercial Payers Play by Different Rules
While Medicare has laid out a clear path, you absolutely cannot assume commercial payers are following it. UnitedHealthcare, Blue Cross, and others operate in their own universes, and assuming they mirror CMS is a recipe for denials. The most effective tool you can have is a simple, payer-specific "cheat sheet."
For your top 5-10 payers, your cheat sheet needs to track these key details:
- Required Modifiers: Does the plan accept the standard Modifier 95, or do they insist on something else like GT or FQ?
- Audio-Only Coverage: Do they reimburse for audio-only sessions (Modifier 93)? And if so, are there strings attached, like for established patients only?
- In-Person Rules: Do they have their own in-person visit requirement? Does it match Medicare's 12-month rule, or is it different?
- Authorization Triggers: Which services, like an initial evaluation (90791) or a therapy session (90837), always need prior authorization when delivered via telehealth?
This simple document, updated every quarter, becomes your front office's bible. It stops costly mistakes before they ever become claims. If you're already buried in rejections, understanding why they happened is the first step to stopping the cycle. Our guide on proactive medical billing denial management can help you build a more resilient revenue cycle.
This level of detail is what separates practices with high first-pass payment rates from those drowning in A/R. It’s about being proactive, not reactive, to secure your revenue and get back to focusing on your patients.
Building Proactive Authorization and Eligibility Workflows
Prior authorization denials are the single biggest, most predictable cash flow killer in mental health. If you’re waiting for a denial to hit your desk before you act, you’re already behind. A reactive approach is just a recipe for write-offs and wasted staff time chasing down payments you should have secured from the start.
Getting this right isn’t about just checking a box. It’s about systematically de-risking every single claim before the session even happens. A simple mistake made by your front office during an eligibility check can be just as costly as a clinician’s coding error.
Create an Authorization Matrix
You need a single source of truth that tells your team exactly what each payer wants. An initial diagnostic evaluation (90791) often has completely different auth rules than a follow-up 60-minute therapy session (90837)—even for the same patient on the same plan.
Your authorization matrix doesn't need to be complicated. Create a simple grid listing your top payers down one side and your most common CPT codes across the top. For each box, fill in the essentials:
- Auth Required? (Yes/No/After X sessions)
- The Trigger: What event requires the auth? Is it always needed for 90791, or only after the fifth session? Does it apply just for out-of-network plans?
- Contact Info: The exact phone number or portal URL for submitting the request.
This simple document stops the guesswork. It turns that one person's "tribal knowledge" into a repeatable process, making sure every telehealth appointment is greenlit for payment.
Script Your Verification Calls
When your staff calls a payer to verify benefits, a generic "Is the patient covered?" just won't cut it. Your team needs a script—a checklist of non-negotiable questions to get the specific details needed for a clean telehealth claim.
Your verification script must include these five questions, every single time:
- Is CPT code [e.g., 90834] a covered benefit for this member?
- Is it covered when delivered via telehealth using Place of Service 10 and Modifier 95?
- Does this service require prior authorization? If it does, what is the auth number?
- How many sessions are approved under that authorization?
- What is the patient’s specific co-pay, co-insurance, and remaining deductible for tele-mental health services?
Giving your team a precise script removes all ambiguity. You get actionable data that dictates exactly how to bill the service—a core principle for getting claims paid on the first pass.
Automate Eligibility Checks in Your EHR
Nobody has time for manual verification calls for every single appointment. Your EHR or practice management system can likely automate these checks for you through its electronic data interchange (EDI) connection.
Set up your system to run an automated eligibility check 24-48 hours before every scheduled appointment. This simple step acts as a safety net, instantly flagging patients whose coverage has lapsed or changed. You catch the problem before it becomes a denial, giving your team time to work it out with the patient.
Managing Retro-Authorizations
Even with the best workflows, you’ll eventually miss one and need to get a retro-authorization. When a service is provided without a required auth, the key is to document every single attempt to get one after the fact.
Log the date, the time, and the name of the representative you spoke with at the insurance company. If they refuse to grant the retro-auth, document the reason they gave you. This log becomes your most powerful tool when appealing the denial, proving you made a good-faith effort to follow their rules. It's a simple step that can mean the difference between getting paid and writing it off.
Creating Audit-Proof Documentation for Telehealth
In the world of telehealth billing, your clinical documentation is your first and only line of defense. When a payer questions a claim, that note is the only evidence you have to prove the service was medically necessary and delivered correctly.
Let's be blunt: generic, copy-pasted notes are an open invitation for audits and recoupments. To get paid and keep the money, every single telehealth note must contain specific elements that justify the claim you submitted. Without them, you leave your practice exposed to costly denials that are nearly impossible to fight.
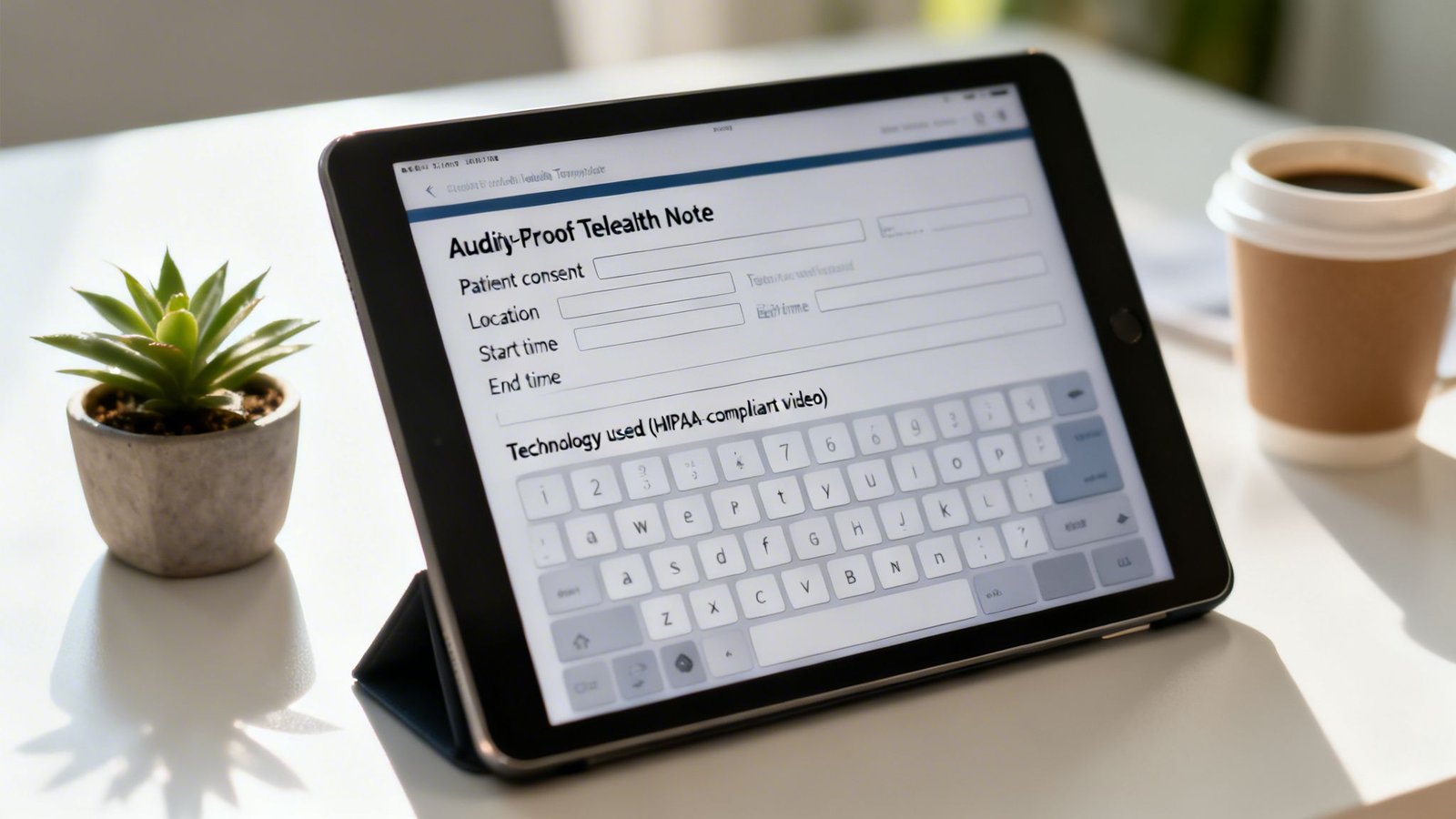
The Anatomy of an Audit-Proof Telehealth Note
Think of this as your pre-flight checklist before signing off on any virtual session. Every telehealth note must be built around a standard template that includes five non-negotiable data points. These are the first things an auditor looks for.
- Patient Consent: A simple statement confirming the patient agreed to telehealth. Something like, “Patient verbally consented to services via synchronous audio-visual telehealth.”
- Patient Location: The physical city and state where the patient was during the session (e.g., “Patient seen at their home in Austin, TX”). This is crucial for confirming compliance with originating site rules.
- Provider Location: Your physical location during the session (e.g., “Provider located at their office in Dallas, TX”). This is non-negotiable for state licensure compliance.
- Technology Used: The platform used for the session, like, “Session conducted via HIPAA-compliant video platform.”
- Start and End Times: The exact times are your primary justification for time-based CPT codes like 90834 or 90837. Document it precisely: “Session started at 10:02 AM and ended at 10:53 AM.”
A note that just says “Telehealth session with patient for 50 minutes” is not defensible. An auditor sees that as a massive red flag, immediately questioning the validity of the service and the CPT code you billed.
Documenting for Different Telehealth Encounters
Not all telehealth services are the same, and your documentation needs to reflect that. A quick check-in requires different details than an intensive therapy session. Here’s a breakdown of what you need to support different service types.
| Documentation Requirements by Telehealth Service Type | ||
|---|---|---|
| Service Type | Example CPT Codes | Key Documentation Elements Required |
| Individual Psychotherapy | 90834, 90837 | Exact start/end times, patient's reported symptoms, specific interventions used (e.g., CBT, DBT), patient's response to treatment, and plan for next session. Must demonstrate a clear "golden thread" from diagnosis to intervention. |
| Psychiatric Diagnostic Evaluation | 90791, 90792 | Comprehensive history, mental status examination, clinical findings, diagnosis (with ICD-10 code), and detailed treatment plan. Must justify the initial assessment. |
| Audio-Only Sessions | 90832, 90834 (with Modifier 93) | All standard elements plus a clear reason for the audio-only format (e.g., "Video connection failed due to poor patient-side internet; session completed via audio-only to ensure continuity of care"). |
| Family Psychotherapy | 90846, 90847 | Identification of all participants present, the focus of the session (e.g., communication patterns, conflict resolution), specific interventions, and progress toward treatment goals. |
The takeaway here is that your documentation must always match the code you're billing. A mismatch is one of the fastest ways to trigger a denial or audit.
Defending Against Medical Necessity Denials
One of the most common and frustrating denials is for "service not medically necessary." This isn't a payer questioning that you had a session; it's questioning why you had it. Payers demand to see a clear "golden thread" that connects the patient's diagnosis and symptoms directly to the treatment you provided in that specific session.
Your note has to explicitly link the plan to the problem.
A weak note says: “Patient reports increased anxiety. Discussed coping skills.”
An audit-proof note says: “Patient reports a 7/10 anxiety level and three panic attacks this week (ICD-10 F41.1). Session focused on practicing diaphragmatic breathing and cognitive restructuring to challenge catastrophic thoughts related to work stressors. Patient demonstrated understanding and will practice these skills daily.”
The second example directly justifies the medical necessity of CPT code 90834. It tells the full story.
Writing Appeal Letters That Actually Win
When a denial hits, your appeal letter needs to be a surgical argument, not an emotional one. The most effective appeals are brief, factual, and use the payer's own rules against them.
First, cite the claim number and denial reason code. Then, methodically dismantle their argument by referencing your own documentation and their clinical policies. For instance, if a claim for CPT 90837 was denied for time:
“This is an appeal for claim #12345, denied for incorrect CPT code. As documented in the attached clinical note, the session began at 2:00 PM and ended at 2:55 PM, for a total duration of 55 minutes. Per AAPC and CPT guidelines, a session of 53 minutes or longer correctly bills to CPT 90837. We request immediate reprocessing and payment.”
This approach removes all subjectivity and forces the reviewer to deal with the facts. For practices needing more specialized support, Happy Billing's expertise in mental health billing ensures your documentation and appeals are always aligned with payer expectations, protecting your revenue.
How Do I Document Patient Consent for Telehealth?
It's simple. Add a standard statement to your note template: "Patient was informed of the risks and benefits of telehealth and verbally consented to treatment via a HIPAA-compliant video platform." Best practice is to also have new patients sign a dedicated telehealth consent form during intake.
What if the Video Connection Fails Mid-Session?
Document it. If a video call drops and you switch to audio-only, your note must reflect what happened and when. For example: "Video connection lost at 15 minutes due to poor patient-side internet; remainder of session completed via audio-only." This detail is critical, especially if the payer requires Modifier 93 for audio-only services.
How Specific Do I Need to Be About Patient and Provider Location?
You must record the city and state for both the patient and provider for every single telehealth encounter. This is non-negotiable. It’s your proof that you are complying with state licensure laws, which generally require the provider to be licensed in the state where the patient is physically located.
H3: How do I bill for audio-only mental health services?
For Medicare, you’ll use the standard CPT code (like 90834), Place of Service 10, and Modifier 93. Crucially, your documentation must explain why a video connection wasn't available or clinically appropriate. Commercial payer rules are all over the map; some Blue Cross plans, for instance, might only cover audio-only for established patients and require a specific modifier like FQ. Always verify the payer’s policy first.
H3: What is the correct Place of Service code for telehealth?
When the patient is at home, the standard code is POS 10. Using the outdated POS 02 is one of the most common and easily avoidable reasons for telehealth denials today. If the patient is at another facility (like a clinic), you would use that facility’s POS code and append the correct telehealth modifier (like 95). For the vast majority of tele-mental health practices, POS 10 is the one you'll use.
H3: Can I bill for a psychiatric evaluation (90791) via telehealth?
Yes, CPT code 90791 (Psychiatric Diagnostic Evaluation) is almost universally approved for telehealth by both Medicare and commercial payers. You should bill it with POS 10 and Modifier 95. Be aware, however, that this initial assessment is a major trigger for prior authorization requirements. Your intake workflow should automatically flag any 90791 to check for auth needs before the appointment is even scheduled to prevent a guaranteed denial.
H3: What happens if state telehealth laws differ from payer rules?
When state law and payer policy don't line up, the payer's policy always wins. The payer is the one cutting the check, so their rules are the ones that matter for getting paid. For example, your state might have a licensure reciprocity law that lets you see a patient in a neighboring state. But if that patient’s Aetna or Cigna plan has a network policy against covering out-of-state providers, your claim will be denied—regardless of what the state allows. In every billing scenario, your provider contract and the payer’s rules dictate what happens to your claim.
At Happy Billing, we turn these complex telehealth rules into your advantage. Our expert team uses a powerful blend of agentic AI and human auditing to hit a 98%+ clean claim rate, making sure you get paid correctly on the first try. Stop chasing down denials and get back to your patients. Visit happybilling.co to see how we do it.