Your Expert Guide to the ICD-10 Code for Weight Loss (2026)
The primary ICD-10 code for weight loss is R63.4 (Abnormal weight loss), but this code must only be used for patients experiencing significant, unintentional weight loss where the underlying cause has not yet been determined. It is a symptom code used to justify the initial diagnostic workup, not a definitive diagnosis for ongoing care or for patients in a supervised weight loss program.
Think of it as the starting point for a diagnostic journey. For practice managers and physician owners, understanding this distinction is critical for preventing claim denials and ensuring proper reimbursement for evaluation and management (E/M) services and diagnostic tests.
Decoding the ICD-10 Code for Abnormal Weight Loss: R63.4

The placement of R63.4 within the ICD-10-CM manual—Chapter 18: "Symptoms, Signs, and Abnormal Clinical and Laboratory Findings, Not Elsewhere Classified"—is a direct instruction on its proper use. This officially classifies R63.4 as a symptom code, a crucial detail for billing and compliance. According to AAPC standards, using a symptom code is the correct and medically necessary way to justify initial workups—such as lab panels, imaging, or specialist referrals—needed to find the underlying pathology. You can find more detail on the code's official classification on the AAPC website.
Payers expect a diagnostic narrative. While R63.4 is perfect for the initial visit, continuing to use it as the primary diagnosis on subsequent claims without a more specific, definitive diagnosis is a direct path to denials for lacking specificity. Payers will not continue to reimburse for a workup that does not lead to a conclusion.
Getting the coding right from the start is fundamental to a healthy revenue cycle. For a deeper dive, check out our expert guide to medical billing for small practices.
Quick Reference for Weight Loss and Related ICD-10 Codes
To help your team navigate these nuances, here is a quick reference table. It breaks down the primary weight loss code and its most common relatives so your practice can select the most precise code every time.
| ICD-10 Code | Description | Primary Use Case |
|---|---|---|
| R63.4 | Abnormal weight loss | Unintentional weight loss where the underlying cause has not yet been determined. |
| R64 | Cachexia | Profound weight loss, muscle wasting, and fatigue associated with a chronic illness like cancer. |
| E43-E46 | Malnutrition | Documented nutritional deficiencies, often used when weight loss is a secondary symptom. |
| F50.0 | Anorexia nervosa | Intentional weight loss driven by a psychological disorder. Requires psychiatric documentation. |
| Z71.3 | Dietary counseling & surveillance | For encounters focused on providing dietary advice, not for diagnosing weight loss itself. |
Think of this table as a cheat sheet for your billing staff and clinicians. Using it helps ensure that what’s documented in the clinical notes lines up perfectly with the code on the claim, minimizing denial risk and keeping your revenue cycle flowing smoothly.
Documentation Requirements For Using R63.4
When it comes to the ICD-10 code for weight loss, R63.4, your clinical documentation is the only thing standing between a paid claim and a swift denial. Payers scrutinize this code heavily, looking for any reason to reject it. The patient's record is the evidence that proves medical necessity for the workup; without a rock-solid case, you are handing revenue back to payers.
A simple note of "weight loss" is a guaranteed red flag for auditors and an easy reason for rejection. You must state that the weight loss was unintentional. This is not optional.
Likewise, vague entries like "patient lost weight" will not get you paid. The note must quantify the loss over a specific timeframe to build a defensible and payable claim.
A note that states, "Patient reports an unintentional 20-pound weight loss over the past 4 months," provides the specific, measurable data that payers need to see. This detail justifies the Evaluation and Management (E/M) service (CPT codes 99202-99215) and any diagnostic tests you order.
Essential Documentation Checklist
To make your claims audit-proof, every note supporting R63.4 must include these key elements. Miss one, and you risk the entire claim.
- Explicit Statement: Clearly document the weight loss as "unintentional" or "involuntary."
- Quantified Amount: Specify the exact amount lost in pounds or as a percentage of body weight (e.g., "15-pound loss," "10% body weight reduction").
- Defined Timeframe: Note the period over which the loss occurred (e.g., "over the past 3 months").
- Associated Symptoms: Record any related symptoms like fatigue, loss of appetite, or pain. This strengthens the clinical picture and justifies the diagnostic investigation.
Following this checklist is the fastest way to build an unimpeachable record and lock in a high first-pass payment rate. To learn more about how detailed notes directly impact your bottom line, you might be interested in our guide on what constitutes a clean claim in medical billing.
Differentiating R63.4 from Related Diagnosis Codes
Claim denials for weight-related issues almost always trace back to one common mistake: confusing the ICD-10 code for weight loss, R63.4, with its look-alike diagnosis codes. Getting this wrong is a fast track to rejections, and the key to getting it right is knowing the specific clinical story each code is meant to tell.
The biggest tripwire is buried in the ICD-10-CM manual’s Excludes1 and Excludes2 notes. These rules are non-negotiable. For example, R63.4 has an Excludes1 note for eating disorders (F50.-). That means you can never code abnormal weight loss alongside a diagnosis like anorexia nervosa (F50.0). Why? Because the eating disorder provides a specific cause, making the symptom code R63.4 incorrect and redundant.
Key Diagnostic Distinctions
It’s just as critical to draw a sharp line between R63.4 and codes for cachexia and malnutrition. They all involve weight loss, but from a clinical and billing perspective, they live in entirely different neighborhoods.
R64 (Cachexia): Reserve this code for the profound weight loss and muscle wasting tied to a severe, underlying chronic illness—think cancer, advanced COPD, or heart failure. Unlike R63.4, which is an unexplained symptom, cachexia points to a known, complex metabolic syndrome. To use R64, the documentation must explicitly link the wasting to that specific chronic disease.
E40-E46 (Malnutrition): These codes flag a state of nutritional deficiency, which is a separate clinical finding from weight loss itself. A patient can have malnutrition confirmed by lab results or clinical assessment without losing significant weight, and vice versa. R63.4 is simply the symptom of weight loss; E40-E46 is a distinct diagnosis.
This decision tree helps visualize the documentation path for using R63.4 correctly.
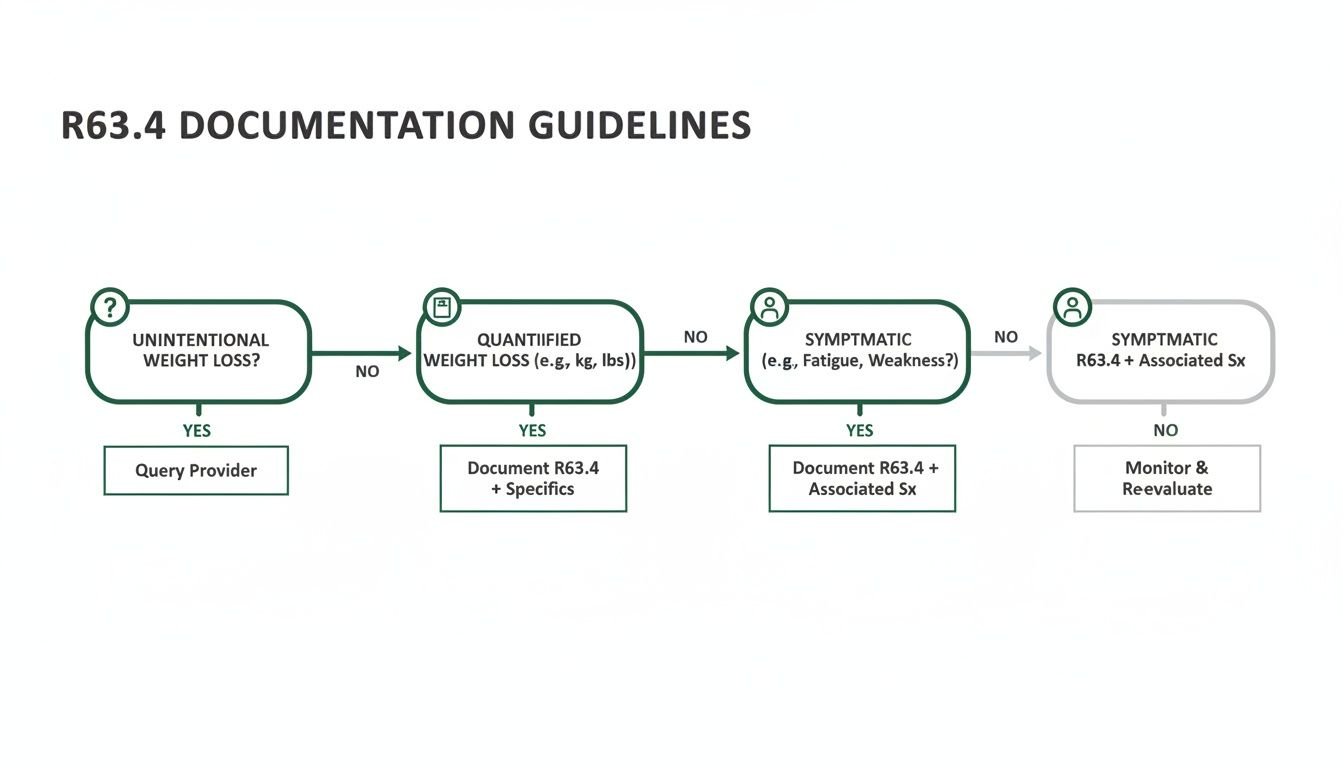
The flowchart makes it clear: R63.4 is only the right choice when the weight loss is unintentional, has been quantified, and the underlying cause is still under investigation. Nailing these distinctions ensures that every claim accurately reflects the patient's clinical reality—a cornerstone of successful billing for our orthopedics billing clients and every other specialty we serve.
Billing for Weight Management with Obesity and BMI Codes

For any medically supervised weight loss program, getting paid hinges on using the right combination of ICD-10 codes. The E66.- series for obesity and overweight conditions is your primary diagnosis, establishing the fundamental medical necessity for the intervention. A patient with morbid obesity, for instance, would be coded with E66.01 (Morbid [severe] obesity due to excess calories).
But an E66 code rarely stands on its own. Payers expect objective data to back it up, and that’s where the Z68.- series for Body Mass Index (BMI) becomes indispensable.
CMS guidelines are clear: pairing a primary diagnosis with supporting data is non-negotiable for many services. To justify preventive medicine counseling (CPT codes 99401-99404), you must link the primary obesity code like E66.01 with a corresponding BMI code, such as Z68.41 (BMI 40.0-44.9, adult).
Justifying Medical Necessity Across Specialties
This coding discipline isn't just for primary care. In orthopedics, a high BMI is a critical factor for proving the medical necessity of major procedures like a total knee replacement. Documenting it with both an E66.- and a Z68.- code creates a rock-solid clinical rationale for surgical intervention.
This simple two-code strategy tells a complete and compelling story to payers, heading off denial risks before they even start. For more tips on building airtight claims, see our resources on RCM for physician practices.
CPT Codes and Payer Rules for Weight Loss Services
Getting paid for weight loss services requires connecting the correct CPT code to the specific ICD-10 diagnosis while adhering to each payer's unique rules. When a patient presents with unintentional weight loss (ICD-10 code R63.4), the visit is a diagnostic workup and should be billed using standard Evaluation and Management (E/M) codes 99202-99215. The specific code level depends on the complexity of medical decision-making.
For a structured, supervised weight management program, the coding strategy changes. Here, the service is justified by a primary obesity diagnosis (E66.- series) supported by a secondary BMI code (Z68.- series).
CPT Codes for Counseling and Behavioral Interventions
Payer policies, particularly from CMS, are strict regarding reimbursement for counseling. To secure payment, claims must be based on a primary diagnosis from the E66.- series and a supporting Z68.- code.
- Preventive Medicine Counseling (99401-99404): These time-based codes are used for counseling patients on risk factors like obesity, where the code level is determined by the duration of the counseling session.
- Health Behavior Assessment & Intervention (96156, 96158, 96159): These codes apply to services from clinical staff addressing psychological or behavioral barriers to managing obesity.
- Medicare Intensive Behavioral Therapy (G0447): This HCPCS code covers 15-minute, face-to-face behavioral counseling sessions for obesity, available to beneficiaries with a BMI ≥ 30 kg/m2. Medicare's coverage rules are highly specific, allowing for one visit every week for the first month, then one visit every other week for months 2-6, and one visit every month for months 7-12 if the patient has lost at least 3kg (6.6 lbs) by the six-month mark.
A common pitfall is billing a significant, separate E/M service on the same day as counseling. You must append Modifier 25 to the E/M code. As detailed in our guide to using CPT Modifier 25, your documentation must prove the E/M visit was a distinct and medically necessary service to prevent the payer from bundling it with the counseling service and denying payment.
Common Denial Traps and How to Avoid Them

When it comes to the ICD-10 codes for weight loss, denials are predictable. Payers frequently reject these claims for the same preventable reasons, slowly chipping away at your practice's bottom line. A proactive defense is the only way to protect your revenue.
The most common tripwire is leaning on the symptom code R63.4 (Abnormal weight loss) for too long. Payers see this code as a starting point, not a final destination. If you use it for the initial workup and then keep using it on subsequent claims without moving to a definitive diagnosis, expect a denial. To them, it looks like a diagnostic dead end.
Insufficient documentation is another guaranteed path to rejection. A claim with R63.4 will get kicked back in a heartbeat if the clinical note is vague. Payers need quantifiable data, not just a casual mention.
A note that just says "patient reports weight loss" is worthless for billing. A defensible, payable note says, "Patient reports an unintentional 15-pound weight loss over the past 3 months." That specificity is what gets you paid.
Key Denial Prevention Tactics
A high clean claim rate doesn’t happen by accident. You have to build a system of proactive checks that catch these errors before they ever leave your office and hit the payer's system.
- Respect the Excludes1 Notes: ICD-10 has hard rules. Pairing R63.4 with an Excludes1 code like F50.0- (Anorexia nervosa) on the same claim is an automatic, computer-generated denial. No human ever sees it; the system just rejects it.
- Build a Smarter Scrubber: Your billing software should be your first line of defense. Configure your claim scrubber with rules that flag these invalid code pairings before they are submitted. Stop the denial before it starts.
- Audit Your Own Work: Don't wait for a payer audit. Routinely pull your own claims that use R63.4. Is the documentation specific enough? Is there a clear plan to find a definitive diagnosis? Fix your own process before a payer forces you to.
Getting these details right will dramatically cut down on rejections and protect your cash flow. To take your revenue cycle defense to the next level, dig into our complete guide on advanced medical billing denial management.
What is the correct ICD-10 code for unintentional weight loss?
The correct code is R63.4 (Abnormal weight loss). This code is specifically for situations where a patient has lost a significant amount of weight without trying, and the underlying cause is not yet known. It should be used to justify the initial diagnostic workup but must be replaced with a more definitive diagnosis on subsequent claims once the cause is identified.
Can I bill CPT code 99401 with an R63.4 diagnosis?
No, this is an incorrect code pairing that will lead to a denial. R63.4 signifies an undiagnosed problem, while CPT code 99401 (Preventive medicine counseling) is for managing established risk factors. To bill for obesity counseling with CPT codes 99401-99404, the primary diagnosis must be from the E66.- series (Overweight and obesity), supported by a secondary Z68.- code for BMI, as per CMS and most commercial payer guidelines.
How do I code for Medicare's Intensive Behavioral Therapy for Obesity?
To bill for Medicare's Intensive Behavioral Therapy for Obesity, use HCPCS code G0447. The service must be face-to-face and last at least 15 minutes. Crucially, the patient must have a BMI of 30 kg/m2 or greater, and this must be documented with an E66.- diagnosis code and a corresponding Z68.- BMI code. Adherence to Medicare’s frequency limitations (weekly for month one, bi-weekly for months 2-6, etc.) and weight loss benchmarks is mandatory for continued reimbursement.