GY Modifier Meaning: Medicare Exclusions & Usage
If your team keeps seeing Medicare denials for services you already know are non-covered, the GY modifier is usually the right signal. In medical billing, GY means the item or service is statutorily excluded from Medicare, so the claim should deny automatically and move cleanly to patient billing or secondary billing instead of getting trapped in the wrong denial workflow.
That distinction matters more than most practices realize. Used correctly, GY is not just a definition problem. It is a routing tool for revenue. It tells Medicare, your billers, and downstream payers that this claim belongs in the statutory exclusion lane, not the medical necessity lane.
What Does the GY Modifier Mean in Medical Billing
A common version of this problem looks like this: a provider performs a service that Medicare does not cover by law, the claim goes out without the right modifier, and staff lose time chasing a denial that was always inevitable.
The gy modifier meaning is simple. It is a two-character HCPCS Level II modifier appended to a CPT or HCPCS code to show the service is statutorily excluded from Medicare. That means it does not meet the definition of a Medicare benefit and will be denied regardless of documentation or appeal effort.
This is why experienced billing teams do not treat GY as a failure. They use it intentionally. If the service is excluded by statute, the goal is to create a predictable Medicare denial so the practice can bill the patient or move the claim to a secondary payer with the right paper trail.
What GY does operationally
GY works best when the practice decides early that the service is outside Medicare’s benefit structure.
That changes the workflow in three ways:
- It prevents wasted rework: Staff do not build an appeal package for a service Medicare can never cover.
- It clarifies responsibility: The denial creates a clean handoff to patient billing or coordination of benefits.
- It keeps edits consistent: Claim scrubbers can separate excluded services from medical necessity denials before submission.
For teams that want a stronger foundation in front-end and back-end claim handling, this guide on medical billing complexities explained is a useful companion.
Practical takeaway: If the service is never a Medicare benefit, your job is not to “win” payment from Medicare. Your job is to route the claim correctly on day one.
Understanding Statutory Noncoverage in Detail
The key to using GY correctly is understanding statutory noncoverage. This is a legal exclusion, not a documentation issue.
A simple way to explain it to staff is this: some services are not on Medicare’s list at all. Others are on the list but may be denied in a specific case. GY belongs only in the first category.

Per this explanation of GA, GX, GY, and GZ modifier use, the GY modifier is a HCPCS Level II code used to indicate an item or service is statutorily excluded from Medicare, meaning it does not meet the definition of any Medicare benefit. The same source notes that Medicare processes over 1.1 billion claims annually and that improper modifier application contributes to 15-20% of denials in high-stakes practices.
Services that often fall into the GY lane
Practice managers usually encounter GY in service categories such as these:
- Routine dental care: Cleanings and similar routine dental services are classic statutory exclusions.
- Routine eye care: Routine eye exams are often used as a straightforward training example for front-desk and billing teams.
- Cosmetic services: A code such as CPT 15823 may be covered in some medically necessary circumstances, but when the service is purely cosmetic, it belongs in a different coverage conversation and may fit the GY pathway.
- Personal comfort items: HCPCS A9270 is commonly reviewed in non-covered item workflows.
- Ambulance exclusions: The same source specifically cites HCPCS A0888 as an example of non-covered ambulance mileage.
What statutory exclusion is not
It is not the same as “Medicare thinks the service was unnecessary today.”
That second scenario involves coverage rules, diagnosis support, and ABN handling. Statutory exclusion is more basic. The Social Security Act excludes the service category itself.
For managers tightening denial prevention, medical billing denial management becomes easier when your team trains around this single question first: Is this service outside the Medicare benefit by law, or is it potentially covered with the right medical necessity support?
GY vs GA and GZ A Clear Comparison for Modifiers
Most GY mistakes happen because teams confuse statutory exclusion with expected medical necessity denial. That error creates the wrong downstream work. It also delays patient billing and secondary submission.
The cleanest way to compare these modifiers is to look at denial reason, ABN handling, and liability.
According to this guide on billing with GY, GA, and GZ modifiers, GY signals a statutory exclusion and automatically triggers denial without requiring an ABN. The same source states that this predictable denial pathway can reduce Days in A/R by 15-30 days compared with using GZ incorrectly for a statutory exclusion and waiting through the wrong denial cycle.
The operational difference
A billing office should think about these modifiers this way:
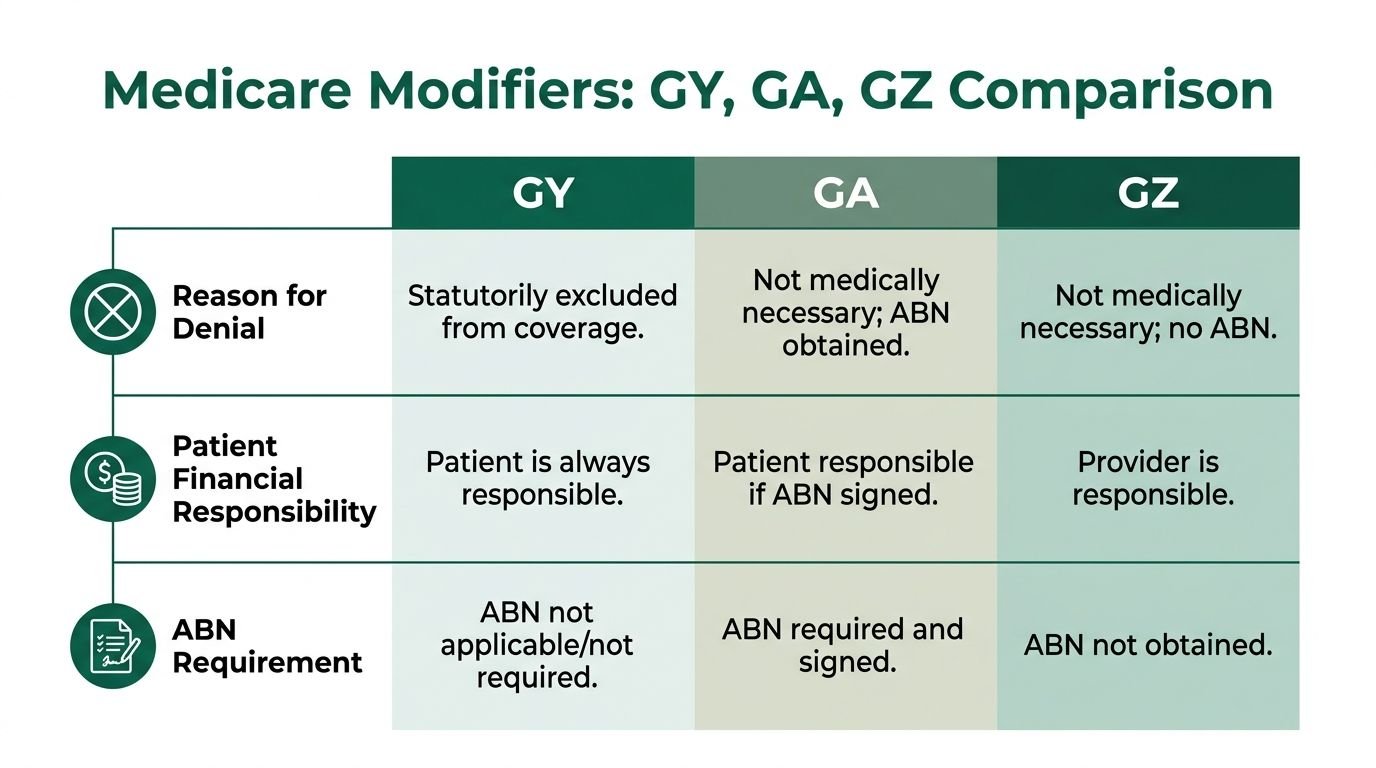
- GY is for services Medicare never covers under the statute.
- GA is used when coverage may be denied for medical necessity and the ABN process has been handled.
- GZ is the problem modifier in many audits because it reflects expected denial without an ABN on file.
If your team puts GZ on a service that should have been billed with GY, you have created extra friction for no gain. The denial may still happen, but it follows the wrong path.
Modifier Comparison GY vs GA vs GZ
| Modifier | Meaning | ABN Required? | Patient Liability |
|---|---|---|---|
| GY | Statutorily excluded service | No | Patient liability shifts after Medicare denial for the excluded service |
| GA | Service may be denied for medical necessity, ABN obtained | Yes | Patient liability depends on valid ABN process |
| GZ | Service expected to deny for medical necessity, no ABN on file | No ABN obtained | Provider risk is higher because ABN protection is missing |
What works and what does not
What works:
- Billing GY on an excluded CPT or HCPCS line.
- Training staff that ABN workflow is not the decision point for statutory exclusions.
- Building claim edits that separate statutory exclusions from medical necessity cases before submission.
What does not:
- Treating every likely Medicare denial as a GZ case.
- Letting staff use GA, GY, and GZ interchangeably.
- Sending excluded services into appeal queues.
A related modifier discipline issue shows up in professional versus technical component billing. This breakdown of modifier 26 vs TC is useful if your team is also tightening coding logic across diagnostic and procedural claims.
Best rule for supervisors: Ask one question before the claim drops. “Is this service excluded by law, or denied because Medicare may not see it as necessary?” The answer determines the modifier family.
How to Use the GY Modifier on a Claim Example
Take a podiatry-style scenario. A Medicare patient receives CPT 11719 for trimming of nondystrophic nails, but there is no qualifying systemic condition or covered exception supporting Medicare payment. In this scenario, many teams either hold the charge or send it out without a clear denial strategy.
The cleaner move is to bill the service with GY.
Sample line-item logic
A simplified claim line may look like this:
| CPT or HCPCS | Modifier | Charge status intent |
|---|---|---|
| 11719 | GY | Submit to Medicare for formal denial of statutorily excluded service |
The point is not reimbursement from Medicare. The point is adjudication.
What the team should expect back
After submission, Medicare should return a denial. In many billing systems, staff then review the ERA or EOB for non-covered adjudication and patient responsibility routing.
A practical remittance review usually includes:
- Confirm primary adjudication happened: The claim should not remain in suspense or RTP status.
- Identify the non-covered denial language: Teams often look for non-covered charge handling on the remittance.
- Route the account correctly: Move it either to patient billing or to the secondary payer workflow.
Many billers are trained to look for remittance patterns such as CARC 96 for non-covered charges when reviewing denied services. The exact remittance details can vary by system and payer setup, so the stronger operational rule is to confirm that Medicare adjudicated the line as non-covered and that your next step is triggered automatically.
Where teams lose money
The failure point is rarely the modifier itself. It is what happens after denial.
Common breakdowns include:
- The claim sits in a generic denial bucket instead of moving to patient or COB follow-up.
- Staff reopen medical necessity review even though the issue is statutory exclusion.
- The EOB never gets attached to the secondary claim.
Use GY as a workflow trigger, not just a coding label. In a strong revenue cycle, the modifier determines the next queue before the ERA arrives.
Payer Implications and Secondary Billing Strategy
The most important part of GY often happens after Medicare denies the claim. In this stage, many practices leak cash.
For services that are statutorily excluded, the Medicare denial is often the document the next payer needs. As noted in this discussion of billing instructions for Medicare modifiers, the Medicare EOB is essential when submitting a GY-denied claim to a commercial secondary payer, and missing coordination of benefits documentation can push A/R beyond 45 days.
Why secondary claims fail
In cardiology and orthopedics, this problem shows up fast.
A claim may be denied correctly by Medicare with GY, but the secondary payer then rejects it because the practice failed to include proof that primary Medicare adjudicated the line. In practical terms, the team did the hard part and missed the handoff.
Examples where managers should watch closely:
- Cardiology: A non-covered diagnostic service or excluded screening-related line needs the Medicare EOB before the secondary payer will process it.
- Orthopedics: Non-covered hardware or excluded line items inside a larger episode can create confusion if the billing team does not split covered and excluded services cleanly.
- Multi-specialty groups: Shared denial teams often misclassify GY-denied accounts as write-offs when they should move to secondary billing.
A better denial segmentation model
High-performance billing offices usually separate these claims into distinct queues:
| Queue | What belongs there | Next action |
|---|---|---|
| Statutory exclusion queue | GY-denied claims | Bill patient or submit to secondary with Medicare adjudication |
| Medical necessity queue | GA or GZ-related denials | Review ABN status, medical records, and appeal options |
| True registration or COB error queue | Eligibility or payer sequencing mistakes | Correct demographics and rebill |
That separation keeps your denial team from treating every denial like an appeal candidate.
For specialty-specific reimbursement complexity, the insurance reimbursement strategies resource helps frame payer sequencing more effectively, and cardiology leaders can also review the dedicated cardiology billing page for procedural billing context.
Documentation Best Practices to Prevent Errors
The strongest GY process starts before charge entry. If the front desk, clinical team, and billing office all identify statutory exclusions the same way, denials become planned events instead of cleanup projects.
A simple internal GY checklist is one of the highest-value controls a practice can build.
What the checklist should include
- Service review: Is the line item a CPT or HCPCS service that Medicare excludes by statute?
- Coverage distinction: Is this non-covered by law, or is it a medical necessity issue?
- Account flagging: Has the EHR or practice management system marked the service for GY handling before claim generation?
- Patient communication: Has staff explained expected financial responsibility clearly and documented that conversation?
- Post-denial routing: Will the account move automatically to patient billing or COB follow-up?
Why documentation still matters
Medicare does not need a medical necessity defense for a statutorily excluded service. Your practice still needs internal documentation.
That documentation protects you when:
- a patient disputes the balance,
- a secondary payer asks for proof of primary adjudication,
- staff question why no ABN was collected.
If your current process produces too many preventable edits, this article on what is a clean claim in medical billing is worth sharing with operations and billing supervisors.
The best GY workflow is boring. Staff identify the service early, code it correctly, get the denial quickly, and move the balance to the right payer or patient without debate.
Frequently Asked Questions About the GY Modifier
Can you use the GY modifier on both CPT and HCPCS codes
Yes. GY is appended to CPT or HCPCS procedure codes when the service or item is statutorily excluded from Medicare. The key is not the code set. The key is whether the service falls outside the Medicare benefit by law.
Does the GY modifier require an ABN
No. For statutory exclusions, an ABN is not required. That is one of the clearest distinctions between GY and modifiers tied to medical necessity denial workflows.
Should a practice appeal a claim denied with GY
Usually, no. A GY denial is expected when the service is excluded by statute. In most cases, the better move is to bill the patient or submit to the secondary payer with the Medicare adjudication record.
Can GY be used with secondary insurance workflows
Yes, and that is where many practices recover revenue they would otherwise write off. The key is to send the secondary payer the Medicare EOB or other required coordination of benefits documentation so the secondary plan can see that the primary payer adjudicated the claim.
Happy Billing helps specialty practices turn modifier decisions into faster cash flow, cleaner denial routing, and tighter payer follow-through. If your team is struggling with Medicare exclusions, secondary billing handoffs, or specialty-specific denial patterns, Happy Billing can build a workflow that fits your existing EHR and keeps excluded services from becoming avoidable A/R.