Anesthesia Modifier Guide for Practice Owners
Anesthesia modifiers are the codes that tell the payer who delivered the anesthesia service and under what supervision model, and they directly determine reimbursement. Get one wrong, and you can turn a properly payable case into a 50% payment, a 3 base unit payment under AD, or a denial.
If your anesthesia volume is steady but collections feel inconsistent, modifier logic is one of the first places to look. In anesthesiology, revenue leakage usually doesn't start with a dramatic coding failure. It starts with small operational misses: the wrong concurrency modifier, a MAC claim missing QS, or documentation that doesn't prove which provider was involved at each point in the case. For an owner, that means lower cash collections, more rework, and A/R that stretches because the claim was technically billable but not payable as submitted.
What Is an Anesthesia Modifier
An anesthesia modifier is a payer-facing signal attached to an anesthesia claim that identifies the provider role and supervision structure behind the case. In practical terms, it tells the payer whether the anesthesiologist personally performed the service, medically directed another provider, or medically supervised too many concurrent cases to qualify for more favorable payment logic.
That sounds administrative. It isn't.
For an anesthesia practice, the modifier often determines whether the claim matches the staffing model you used in the OR, GI suite, or ASC. If the modifier doesn't match the documented reality, the payer doesn't just see a typo. The payer sees a claim that may be overbilled, under-supported, or not payable under that plan's rules.
Why owners should care
Most practice owners look first at case volume, facility relationships, and payer contracts. Those all matter. But modifier discipline is one of the fastest ways to protect the revenue you've already earned.
A busy group can still underperform financially if its claims don't reflect concurrency, provider relationship, and MAC status correctly. That's why anesthesia billing is less forgiving than many other specialties. The modifier isn't a side note on the claim. It's part of the payment decision itself.
Practical rule: If your staffing model changes faster than your billing workflow can capture it, your modifier process is already a financial risk.
There's also a historical reason anesthesiology ended up this tightly coded. The specialty traces back to the public ether demonstration at Massachusetts General Hospital on October 16, 1846, followed by James Young Simpson's adoption of chloroform in 1847, milestones that helped turn anesthesia into a distinct medical discipline whose services are now differentiated on claims by provider role and supervision model, as reflected in modifier-driven billing logic such as AA, QK, QX, QY, QZ, AD, and others according to this history of anesthesia's development into a modern specialty.
If you want a broader refresher on anesthesia procedure coding before looking at modifier strategy, this guide to anesthesia CPT code fundamentals is a useful starting point.
Why Anesthesia Modifiers Uniquely Impact Revenue
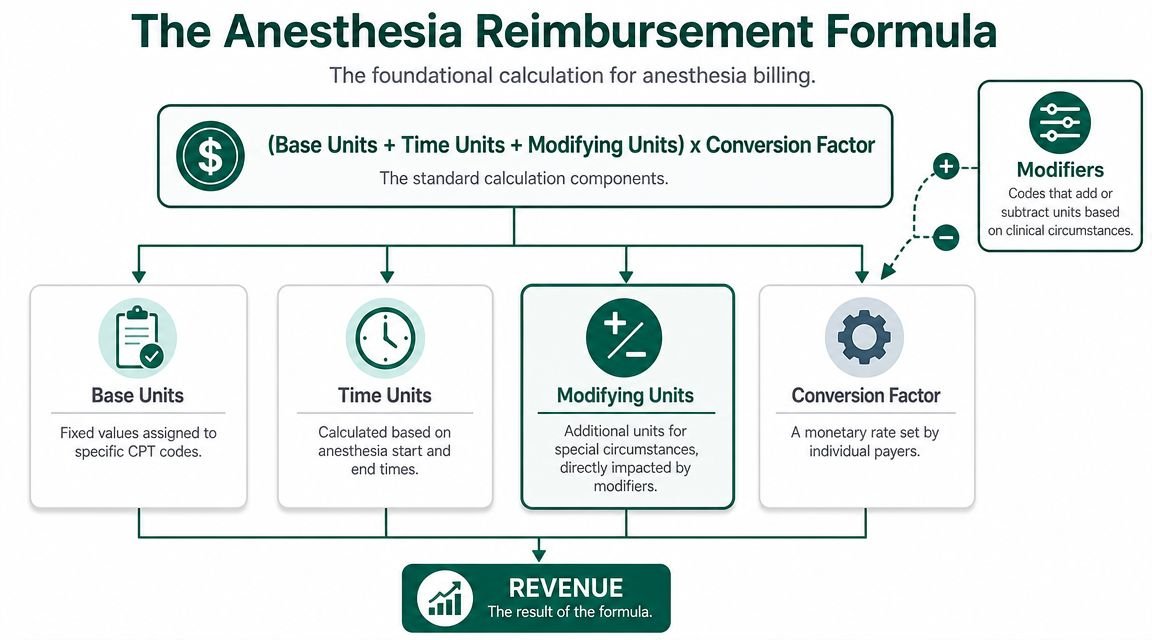
Anesthesia billing is unusual because the claim value isn't driven only by the procedure code. Payment depends on units, time, and payer logic, and the modifier changes how the payer applies that logic to the case.
Modifiers are payment controls, not labels
Owners sometimes assume modifiers are descriptive, like an annotation that helps the payer understand the chart. In anesthesia, that's the wrong mental model. The modifier is one of the payer's primary controls for deciding how much of the claim is payable and to whom.
A payer policy from Moda Health spells this out clearly. QK applies when an anesthesiologist medically directs 2 to 4 concurrent anesthesia procedures. AD applies when the physician medically supervises more than 4 concurrent procedures. The same policy states that AD is reimbursed at only 3 base units per procedure, and QX is reimbursed at 50% of the applicable fee schedule rate for CRNA services under physician medical direction, as outlined in this anesthesia payment modifier policy.
That is the business issue in one paragraph. If your documentation supports one modifier but the claim goes out with another, payment can change immediately.
Where the revenue damage shows up
The damage usually lands in three places:
- Allowed amount compression because the payer adjudicates the claim under a lower-paying supervision model.
- Denial and rebill work because the modifier doesn't match concurrency or provider role.
- A/R drag because staff now have to reconstruct timing, staffing, and chart support after the fact.
Here's the operational takeaway. In anesthesia, the same case can move through entirely different reimbursement paths depending on whether the physician was personally performing, medically directing, or medically supervising. That means your charge capture process has to reflect real staffing conditions, not assumptions carried over from the schedule.
A strong anesthesia revenue cycle doesn't just post charges quickly. It captures who did what, when they did it, and how many rooms were running at the same time.
Practices that need a deeper operational view of anesthesia revenue workflows often benefit from comparing their front-end documentation and post-op charge process against a specialty-specific anesthesia medical billing services framework.
Decoding Common Modifiers and Their Financial Impact
Most anesthesia modifier guides stop at definitions. Owners need the financial meaning of each one. The question isn't just “What does this code mean?” It's “What happens to reimbursement if we choose it, and can our chart support it?”
Personally performed and directed models
When the anesthesiologist personally performs the case, the claim typically uses AA. Financially, that matters because you're telling the payer this wasn't a direction or supervision scenario. The physician personally provided the anesthesia service.
When a physician medically directs 2, 3, or 4 concurrent anesthesia procedures, QK applies. When the physician medically directs one qualified non-physician anesthetist, QY applies. These are not interchangeable staffing labels. They represent different provider relationships, and payers expect the record to support the exact model billed.
For the non-physician side, QX identifies CRNA service under physician medical direction. Under the Moda policy cited earlier, QX is reimbursed at 50% of the applicable fee schedule rate. That's why the physician-side and CRNA-side modifiers have to align with the actual staffing structure, not just the schedule template.
Supervision and MAC modifiers
AD is the modifier owners should watch carefully in high-volume environments. It applies when the physician medically supervises more than 4 concurrent anesthesia procedures. Under the same payer policy, reimbursement is limited to 3 base units per procedure. That creates an immediate financial drop compared with a properly documented medical direction scenario. If your group regularly stretches staffing, this isn't a coding footnote. It's margin pressure.
For monitored anesthesia care, modifier logic becomes a separate compliance issue. QS identifies the MAC service itself. CMS also states that G8 is reserved for MAC associated with certain deep, complex, complicated, or markedly invasive surgical procedures on specific anesthesia codes only. When those listed codes are used and MAC is provided, QS must be reported, according to this CMS article on MAC coding requirements.
That means a MAC claim can fail even when the clinical service was appropriate, because the modifier combination didn't match the underlying anesthesia code.
Common anesthesia modifiers and reimbursement impact
| Modifier | Scenario | Typical reimbursement impact |
|---|---|---|
| AA | Anesthesiologist personally performs the service | Payment follows the personally performed path if documentation supports it |
| QK | Physician medically directs 2 to 4 concurrent procedures | Payment follows medical direction rules and depends on payer policy |
| QY | Physician medically directs one qualified non-physician anesthetist | Payment follows one-to-one medical direction rules and payer edits |
| QX | CRNA service under physician medical direction | Under the Moda policy, paid at 50% of the applicable fee schedule rate |
| AD | Physician medically supervises more than 4 concurrent procedures | Under the Moda policy, paid at 3 base units per procedure |
| QS | Monitored anesthesia care | Identifies MAC service and must align with underlying code and payer rules |
| G8 | MAC for certain deep, complex, complicated, or markedly invasive procedures | Valid only on certain anesthesia codes under CMS guidance |
One practical point for owners with mixed-specialty claim patterns. Modifier discipline in anesthesia is its own world, and it shouldn't be handled with the same shortcuts people use in general procedural billing. If your internal team tends to treat modifiers generically, even a common educational reference like this overview of modifier 59 usage is a reminder that modifier strategy is specialty-specific and financially sensitive.
Real-World Scenarios and Revenue Consequences
The fastest way to understand the value of an anesthesia modifier is to compare two versions of the same case. The procedure and provider effort may look similar clinically, but the payer's result can change materially based on modifier selection and documentation support.
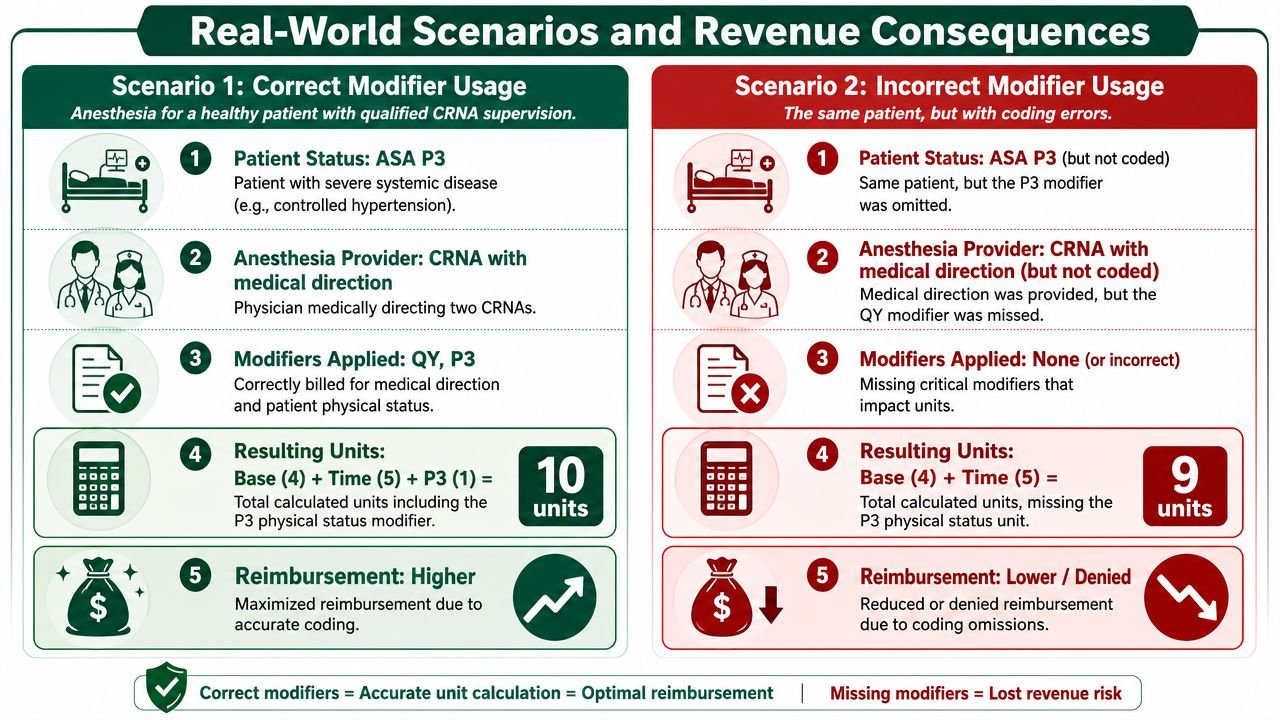
Scenario one with the staffing model captured correctly
Take a routine outpatient surgery day. One anesthesiologist is medically directing qualified personnel across assigned rooms, and the provider documentation supports the direction model used for each case. The physician claim reflects the proper medical direction modifier for that staffing arrangement, and the non-physician claim reflects the corresponding modifier on the CRNA side.
That claim has a chance to adjudicate on the first pass because the payer sees a coherent story. Provider role, concurrency, and case timing line up. No one has to reopen the chart to prove which room counted toward concurrency at a specific moment.
Scenario two with a modifier mismatch
Now take the same clinical service, but the physician is billed as though the case were personally performed, or a directed case is sent without the right corresponding modifier on the CRNA side. The payer now sees a conflict between staffing, charting, and billed role.
Two outcomes are common. The payer denies the claim for a modifier error, or it pays under a less favorable logic because the billed supervision structure doesn't qualify. Either way, your staff is now doing expensive cleanup work after the revenue should have been in the bank.
The cost of a bad modifier decision isn't just the initial underpayment. It's the rebill time, the appeal cycle, and the aging that follows.
A MAC example where the denial is avoidable
Monitored anesthesia care is a good example because the denial often comes from process failure, not medical necessity. CMS states that QS identifies MAC, and G8 is limited to certain deep, complex, complicated, or markedly invasive procedures on specific anesthesia codes. When a listed code is used and MAC is provided, QS must be reported.
For an owner, the lesson is simple. If your team treats MAC modifiers as optional add-ons rather than code-dependent requirements, you'll create avoidable denials. The clinical care may be fine. The claim still stalls.
What actually works in practice
The strongest groups don't rely on memory for concurrency and modifier choice. They build workflow around the facts payers need to see.
- Capture provider role at the case level so the charge doesn't depend on someone reconstructing staffing later.
- Reconcile concurrency before claim submission when rooms overlap or handoffs occur.
- Tie MAC review to the underlying anesthesia code so QS and, where applicable, G8 are validated before the claim leaves the system.
- Escalate exceptions the same day when the schedule and the chart don't tell the same story.
What doesn't work is assuming the schedule proves the billing model. Schedules show intent. Payers pay on documentation.
How Payer Rules and Documentation Gaps Cause Denials
Most modifier denials don't come from random data-entry mistakes. They come from a broken system. The practice uses one internal rule for all payers, assumes everyone treats the same modifier the same way, and then discovers too late that the plan's published policy says otherwise.
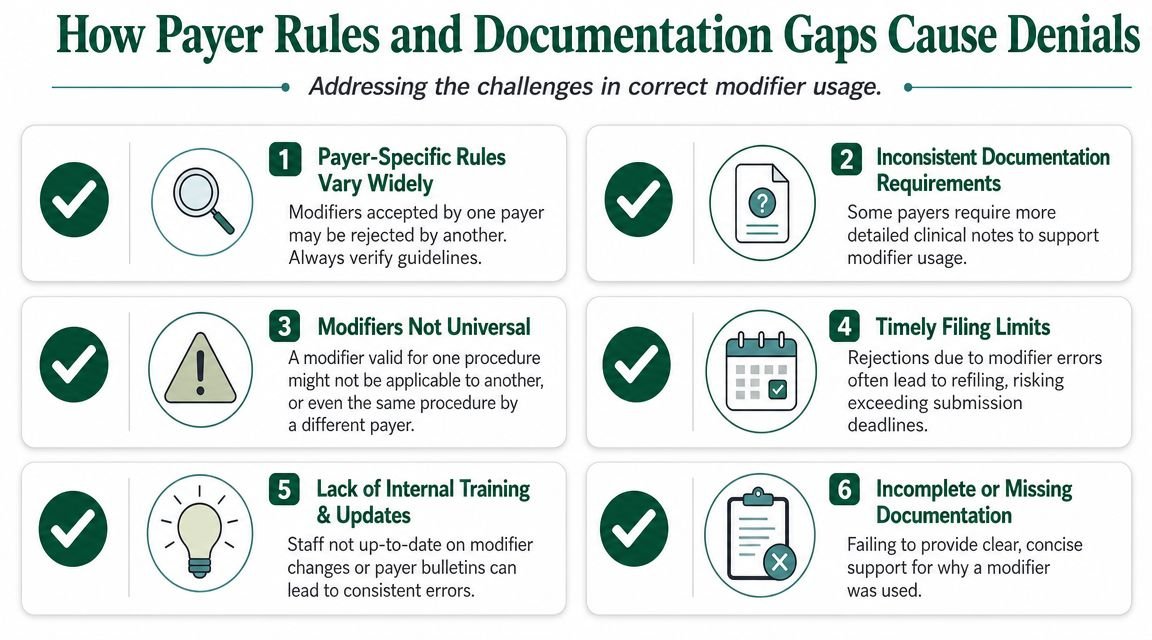
Payer variation is the first denial engine
Horizon NJ Health states that anesthesia claims without the required HCPCS modifier will not be reimbursed. The same policy says AD, QK, QX, and QY are paid at 50% of fee schedule, while QZ is not considered for reimbursement, as described in this Horizon NJ Health anesthesia reimbursement policy.
That's the point owners need to internalize. “Correct” from a coding perspective and “payable” under a specific payer are not always the same operational question. If your billing workflow doesn't maintain a payer-by-payer anesthesia modifier matrix, you will create denials even when the clinical scenario is understood.
Documentation failures are the second denial engine
The other major problem is proof. Payers often treat modifier pathways as mutually exclusive. If the record doesn't establish the exact provider role, time units, and concurrency during the case, the claim becomes vulnerable even when the selected modifier seems reasonable.
This is especially common in high-volume settings where staffing changes mid-case, relief coverage happens, or the documentation lags behind the actual room activity.
Owner takeaway: If your team can't prove concurrency and provider involvement at each moment of the case, the modifier is just an unsupported assertion.
The denial patterns worth auditing first
If you're diagnosing revenue leakage, start with these failure points:
- Missing required anesthesia modifiers on payer plans that won't reimburse without them.
- Concurrency threshold errors where a directed case should have moved into a supervision model.
- Physician and CRNA modifier mismatch between paired claims.
- MAC claims missing QS or using G8 without confirming code-level eligibility.
- Late chart clarification requests that push corrected claims closer to filing deadlines.
Practices that want a cleaner process usually need tighter denial surveillance, not just coder education. A more disciplined medical billing denial management workflow helps surface whether these are isolated claim defects or recurring process failures.
Optimizing Modifiers with Specialized RCM
The fix for anesthesia modifier leakage isn't more memorization. It's building a revenue cycle process that treats modifier selection as a controlled operational decision tied to staffing, documentation, and payer rules.
What a disciplined process looks like
The strongest anesthesia revenue workflows do three things well.
First, they validate provider role before the claim is built. That means the charge capture process reflects whether the physician personally performed, medically directed, or medically supervised, instead of leaving the billing team to infer it later.
Second, they check payer acceptability separately from coding logic. A modifier may fit the clinical story but still trigger edits or different reimbursement treatment under a local plan. That's why practices need a living payer matrix, not a static cheat sheet.
Third, they audit exceptions aggressively. Cases with overlapping rooms, relief coverage, and MAC services are where leakage hides. If your team only reviews denials after they post, you're reacting to lost time and delayed cash.
Why specialized oversight changes the numbers that matter
When modifier logic is handled well, owners usually see the benefit in cleaner first-pass adjudication, fewer preventable denials, and less aged A/R tied to avoidable rework. The gains aren't theoretical. They show up in fewer corrected claims and less back-and-forth over documentation support.
We've seen that the practices that improve fastest are the ones that stop treating anesthesia claims as generic professional billing. They build workflows around concurrency, medical direction, and payer-specific rules from the start.
If you're comparing internal cleanup against outside expertise, this overview of outsourced revenue cycle management helps frame the decision in operational terms instead of vendor language.
Anesthesia Modifier FAQs for Practice Owners
Should I treat modifier issues as a coding problem or a revenue problem
Treat them as a revenue control problem. Coding is only one part of it. If the modifier doesn't reflect the documented staffing model and the payer's rules, the claim either pays incorrectly or doesn't pay at all.
How do I know whether concurrency is costing us money
Look for claims where provider documentation, anesthesia time, and final modifier assignment don't align. ASA-based materials and payer guidance distinguish AD for supervision of more than four concurrent procedures from QK for direction of two to four, and payers can deny when the record doesn't prove exact provider role, time units, and concurrency at each moment, as summarized in this EmblemHealth explanation of anesthesia modifier reporting.
What should I ask my billing team this month
Ask four direct questions:
- Which payers deny anesthesia claims without a modifier
- How are we verifying concurrency before claim submission
- How are we handling MAC claims that require QS and code-level review
- What percentage of anesthesia denials tie back to modifier or documentation mismatch
If the answers are vague, the process probably is too.
Is it worth benchmarking our RCM approach against outside anesthesia resources
Yes. Owners benefit from seeing how other firms think about staffing, claims flow, and denial prevention. For a practical outside perspective, this resource on Optimizing anesthesia practice RCM is worth reviewing alongside your internal workflow. If you want specialty-specific support, you can also see what focused anesthesiology billing services should cover before deciding whether to rebuild your internal process or outsource part of the work.
If your anesthesia modifiers are generating denials, underpayments, or slow-moving A/R, Happy Billing can help you identify where revenue is leaking. A complimentary billing audit will show whether the problem is payer rules, modifier workflow, documentation support, or all three.